

The effects of fructose intake on serum uric acid vary among controlled dietary trials
- PMID: 22457397
- PMCID: PMC3327749
- DOI: 10.3945/jn.111.151951
The effects of fructose intake on serum uric acid vary among controlled dietary trials
Abstract
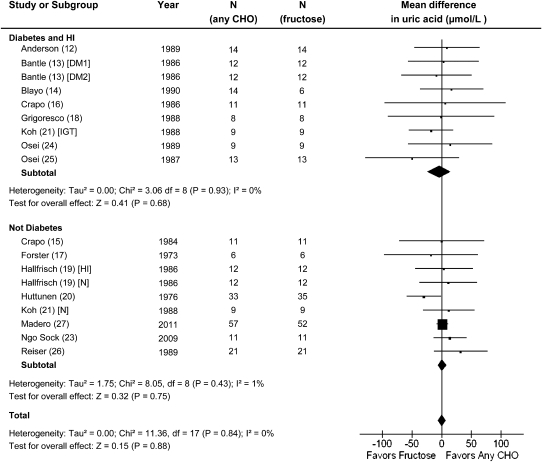
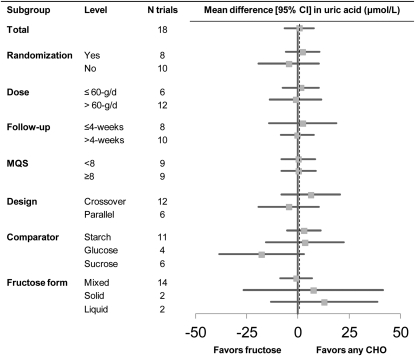
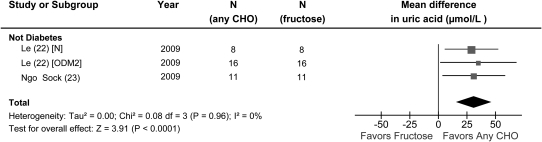
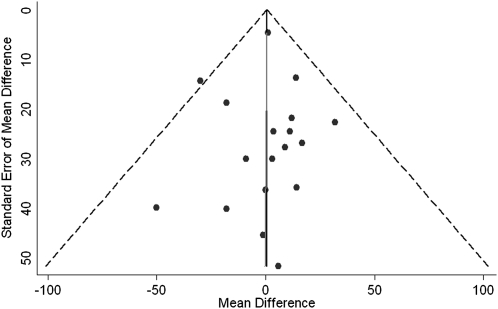
Hyperuricemia is linked to gout and features of metabolic syndrome. There is concern that dietary fructose may increase uric acid concentrations. To assess the effects of fructose on serum uric acid concentrations in people with and without diabetes, we conducted a systematic review and meta-analysis of controlled feeding trials. We searched MEDLINE, EMBASE, and the Cochrane Library for relevant trials (through August 19, 2011). Analyses included all controlled feeding trials ≥ 7 d investigating the effect of fructose feeding on uric acid under isocaloric conditions, where fructose was isocalorically exchanged with other carbohydrate, or hypercaloric conditions, and where a control diet was supplemented with excess energy from fructose. Data were aggregated by the generic inverse variance method using random effects models and expressed as mean difference (MD) with 95% CI. Heterogeneity was assessed by the Q statistic and quantified by I(2). A total of 21 trials in 425 participants met the eligibility criteria. Isocaloric exchange of fructose for other carbohydrate did not affect serum uric acid in diabetic and nondiabetic participants [MD = 0.56 μmol/L (95% CI: -6.62, 7.74)], with no evidence of inter-study heterogeneity. Hypercaloric supplementation of control diets with fructose (+35% excess energy) at extreme doses (213-219 g/d) significantly increased serum uric acid compared with the control diets alone in nondiabetic participants [MD = 31.0 mmol/L (95% CI: 15.4, 46.5)] with no evidence of heterogeneity. Confounding from excess energy cannot be ruled out in the hypercaloric trials. These analyses do not support a uric acid-increasing effect of isocaloric fructose intake in nondiabetic and diabetic participants. Hypercaloric fructose intake may, however, increase uric acid concentrations. The effect of the interaction of energy and fructose remains unclear. Larger, well-designed trials of fructose feeding at "real world" doses are needed.
Conflict of interest statement
Author disclosures: J. L. S. has received consultant fees, travel funding, honoraria, or additional research support from the CIHR, Calorie Control Council, The Coca-Cola Company, Archer Daniels Midland, International Life Sciences Institute (ILSI) North America and Brazil, Abbott Laboratories, and Pulse Canada. R.J.d.S. and J.B. have received additional research support from the CIHR and The Coca-Cola Company. T. M. S. W. is a part owner and the President of Glycemic Index Laboratories, Toronto, Canada and has authored several popular diet books on the glycemic index for which he has received royalties from Phillipa Sandall Publishing Services and CABI Publishers. He has received consultant fees, honoraria, travel funding, or additional research support from or served on the Scientific Advisory Board for CIHR, Canadian Diabetes Association (CDA), Dairy Farmers of Canada, McCain Foods, Temasek Polytechnic, Northwestern University, Royal Society of London, Glycemic Index Symbol program, CreaNutrition AG, McMaster University, Canadian Society for Nutritional Sciences, National Sports and Conditioning Association, Faculty of Public Health and Nutrition--Autonomous University of Nuevo Leon, Diabetes and Nutrition Study Group of the European Association for the Study of Diabetes. C.W.C.K. has received consultant fees, honoraria, travel funding, or additional research support from or served on the Scientific Advisory Board for the CIHR, The Coca Cola Company, Abbott Laboratories, Advanced Food Materials Network, Almond Board of California, American Peanut Council, American Pistachio Growers, Barilla, California Strawberry Commission, Canola Council of Canada, Danone, General Mills, Hain Celestial, International Tree Nut Council, Kellogg, Loblaw Brands Ltd, Oldways, Orafti, Paramount Farms, Pulse Canada, Saskatchewan Pulse Growers, Solae and Unilever. D. J. A. J. has received consultant fees, honoraria, travel funding, or additional research support from or served on the Scientific Advisory Board for the Calorie Control Council, The Coca Cola Company, Barilla, Solae, Unilever, Hain Celestial, Loblaws Supermarkets, Inc., Sanitarium Company, Herbalife International, Pacific Health Laboratories, Inc., Metagenics/MetaProteomics, Bayer Consumer Care, Oldways Preservation Trust, The International Tree Nut Council Nutrition Research & Education, The Peanut Institute, Procter and Gamble Technical Centre Limited, Griffin Hospital for the development of the NuVal System, Soy Advisory Board of Dean Foods, Alpro Soy Foundation, Nutritional Fundamentals for Health, Pacific Health Laboratories, Kellogg's, Quaker Oats, The Coca-Cola Sugar Advisory Board, Pepsi Company, Agrifoods and Agriculture Canada (AAFC), Canadian Agriculture Policy Institute (CAPI), The Almond Board of California, The California Strawberry Commission, Orafti, the Canola and Flax Councils of Canada, Pulse Canada, the Saskatchewan Pulse Growers, and Abbott Laboratories. D. J. A. J. also holds additional grant support from the CIHR, Canadian Foundation for Innovation (CFI), Ontario Research Fund (ORF), and Advanced Foods and Material Network (AFMNet). A. L. J. is a part owner, Vice-President, and Director of Research of Glycemic Index Laboratories, Toronto, Canada. She has received additional research support from the CDA. L. C. is a casual Clinical Research Coordinator at Glycemic Index Laboratories, Toronto, Canada. L.C., V.H., and A.M. received additional research support from the CIHR. D.D.W., A.I.C., M.E.Y., A.J.C., M.D., and L.A.L have no declared conflicts of interest related to this paper.
Figures
References
-
- Ardern CI, Katzmarzyk PT. Geographic and demographic variation in the prevalence of the metabolic syndrome in Canada. Can J Diab. 2007;31:34–46
-
- Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA. 2002;287:356–9 - PubMed
-
- Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM, Smith SC., Jr Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120:1640–5 - PubMed
-
- Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011;63:3136–41 - PubMed
-
- Becker MA, Jolly M. Hyperuricemia and associated diseases. Rheum Dis Clin North Am. 2006;32:275–93 - PubMed
