

Towards endometriosis diagnosis by gadofosveset-trisodium enhanced magnetic resonance imaging
- PMID: 22457748
- PMCID: PMC3310862
- DOI: 10.1371/journal.pone.0033241
Towards endometriosis diagnosis by gadofosveset-trisodium enhanced magnetic resonance imaging
Abstract
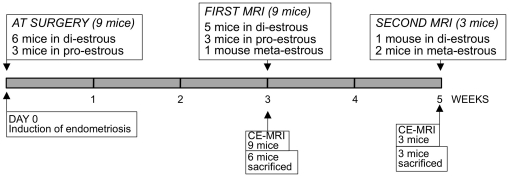
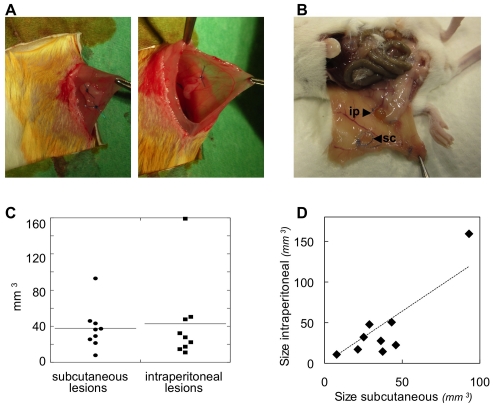
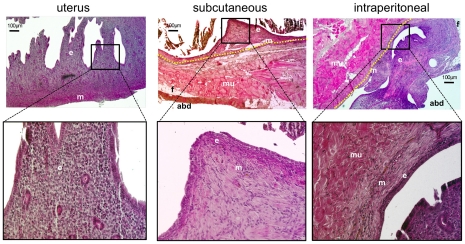
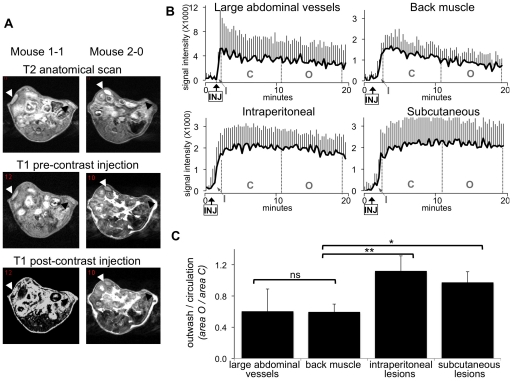
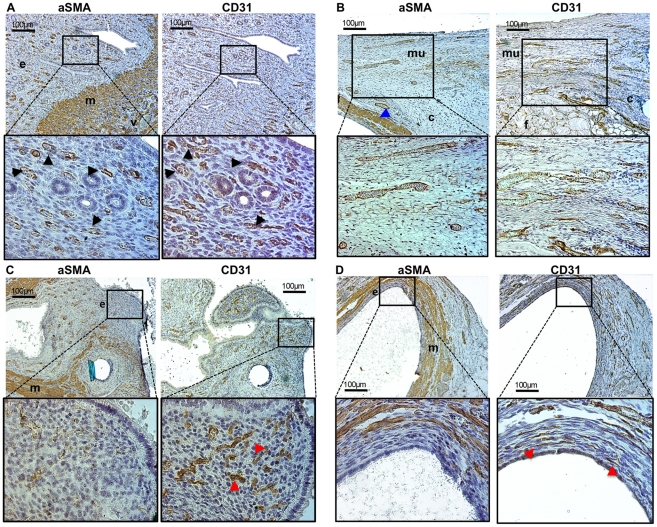
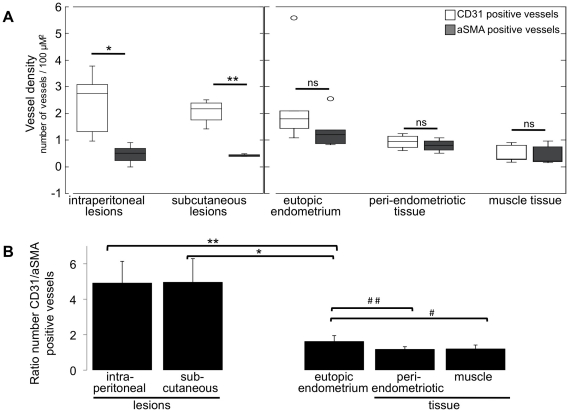
Endometriosis is defined as the presence of endometrial tissue outside the uterus. It affects 10-15% of women during reproductive age and has a big personal and social impact due to chronic pelvic pain, subfertility, loss of work-hours and medical costs. Such conditions are exacerbated by the fact that the correct diagnosis is made as late as 8-11 years after symptom presentation. This is due to the lack of a reliable non-invasive diagnostic test and the fact that the reference diagnostic standard is laparoscopy (invasive, expensive and not without risks). High-molecular weight gadofosveset-trisodium is used as contrast agent in Magnetic Resonance Imaging (MRI). Since it extravasates from hyperpermeable vessels more easily than from mature blood vessels, this contrast agent detects angiogenesis efficiently. Endometriosis has high angiogenic activity. Therefore, we have tested the possibility to detect endometriosis non-invasively using Dynamic Contrast-Enhanced MRI (DCE-MRI) and gadofosveset-trisodium as a contrast agent in a mouse model. Endometriotic lesions were surgically induced in nine mice by autologous transplantation. Three weeks after lesion induction, mice were scanned by DCE-MRI. Dynamic image analysis showed that the rates of uptake (inwash), persistence and outwash of the contrast agent were different between endometriosis and control tissues (large blood vessels and back muscle). Due to the extensive angiogenesis in induced lesions, the contrast agent persisted longer in endometriotic than control tissues, thus enhancing the MRI signal intensity. DCE-MRI was repeated five weeks after lesion induction, and contrast enhancement was similar to that observed three weeks after endometriosis induction. The endothelial-cell marker CD31 and the pericyte marker α-smooth-muscle-actin (mature vessels) were detected with immunohistochemistry and confirmed that endometriotic lesions had significantly higher prevalence of new vessels (CD31 only positive) than the uterus and control tissues. The diagnostic value of gadofosveset-trisodium to detect endometriosis should be tested in human settings.
Conflict of interest statement
Figures
References
-
- Groothuis PG, Nap AW, Winterhager E, Grummer R. Vascular development in endometriosis. Angiogenesis. 2005;8:147–56. - PubMed
-
- Simoens S, Hummelshoj L, D'Hooghe T. Endometriosis: cost estimates and methodological perspective. Hum Reprod Update. 2007;13:395–404. - PubMed
-
- Vigano P, Parazzini F, Somigliana E, Vercellini P. Endometriosis: epidemiology and aetiological factors. Best Pract Res Clin Obstet Gynaecol. 2004;18:177–200. - PubMed
-
- Simoens S, Hummelshoj L, Dunselman G, Brandes I, Dirksen C, et al. Endometriosis cost assessment (the EndoCost study): a cost-of-illness study protocol. Gynecol Obstet Invest. 2011;71:170–6. - PubMed
-
- de Graaff AA, Dunselman GA, Delvoux B, van Kaam KJ, Smits LJ, et al. B lymphocyte stimulator −817C>T promoter polymorphism and the predisposition for the development of deep infiltrating endometriosis. Fertil Steril. 2010;94:1108–10. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
