

Regional brain structural dysmorphology in human immunodeficiency virus infection: effects of acquired immune deficiency syndrome, alcoholism, and age
- PMID: 22458948
- PMCID: PMC3393798
- DOI: 10.1016/j.biopsych.2012.02.018
Regional brain structural dysmorphology in human immunodeficiency virus infection: effects of acquired immune deficiency syndrome, alcoholism, and age
Abstract
Background: Human immunodeficiency virus (HIV) infection and alcoholism each carries liability for disruption of brain structure and function integrity. Despite considerable prevalence of HIV-alcoholism comorbidity, few studies examined the potentially heightened burden of disease comorbidity.
Methods: Participants were 342 men and women: 110 alcoholics, 59 with HIV infection, 65 with HIV infection and alcoholism, and 108 healthy control subjects. This design enabled examination of independent and combined effects of HIV infection and alcoholism along with other factors (acquired immune deficiency syndrome [AIDS]-defining events, hepatitis C infection, age) on regional brain volumes derived from T1-weighted magnetic resonance images.
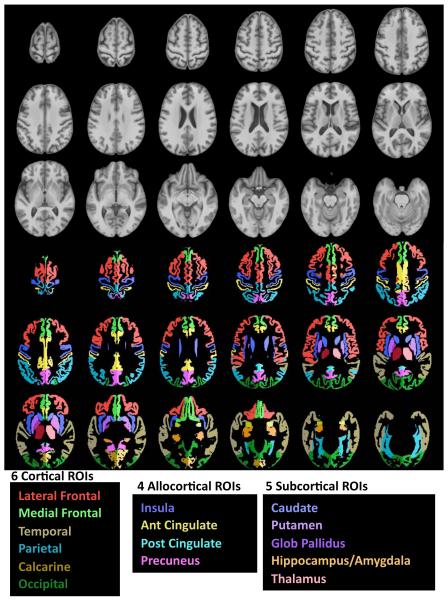
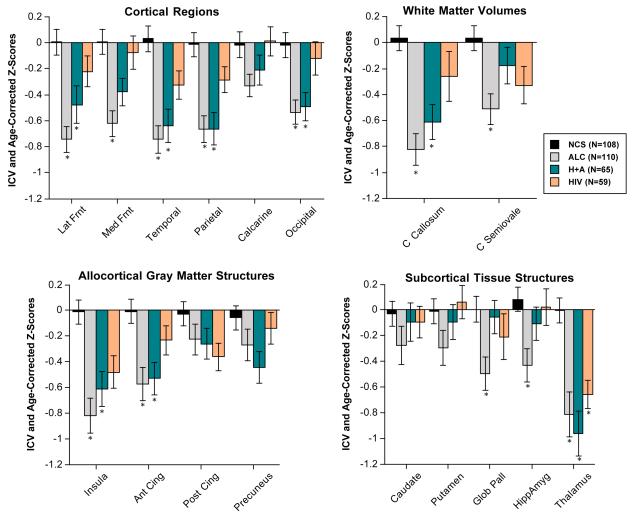
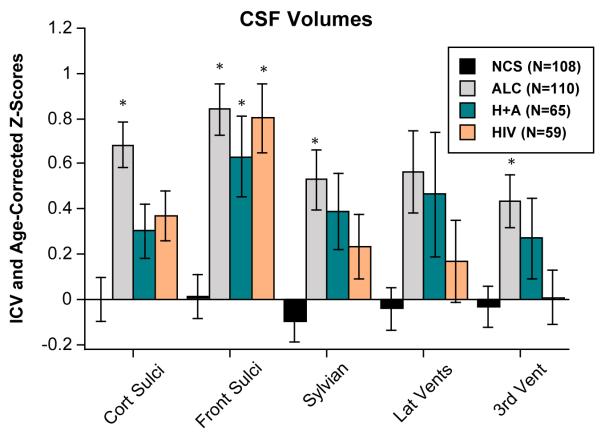
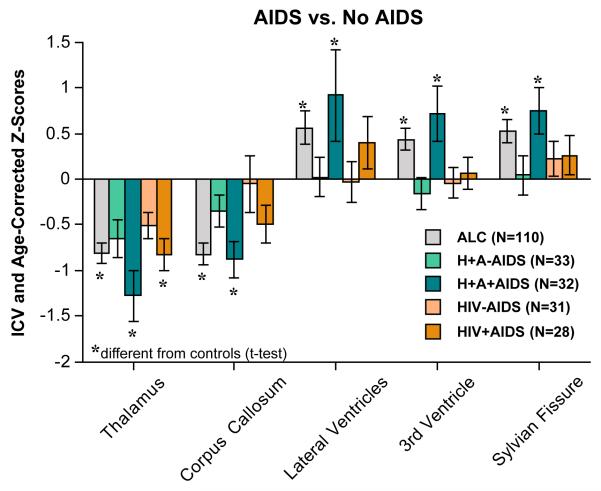
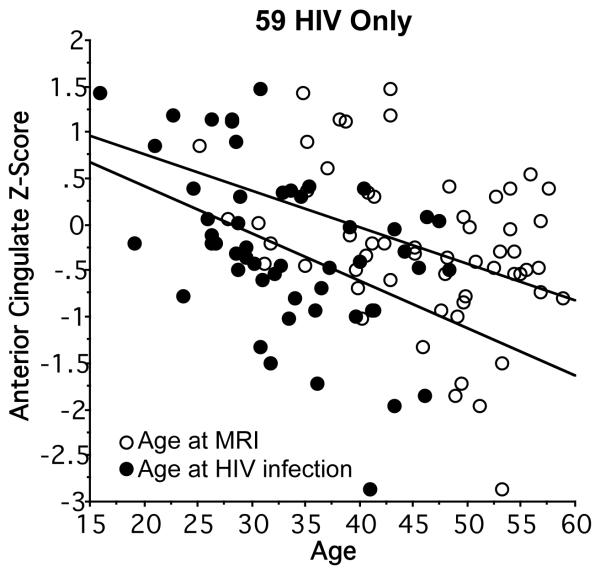
Results: Brain volumes, expressed as Z scores corrected for intracranial volume and age, were measured in 20 tissue and 5 ventricular and sulcal regions. The most profound and consistent volume deficits occurred with alcohol use disorders, notable in the cortical mantle, insular and anterior cingulate cortices, thalamus, corpus callosum, and frontal sulci. The HIV-only group had smaller thalamic and larger frontal sulcal volumes than control subjects. HIV disease-related factors associated with greater volume abnormalities included CD4 cell count nadir, clinical staging, history of AIDS-defining events, infection age, and current age. Longer sobriety and less lifetime alcohol consumption were predictive of attenuated brain volume abnormalities in both alcohol groups.
Conclusions: Having HIV infection with alcoholism and AIDS had an especially poor outcome on brain structures. That longer periods of sobriety and less lifetime alcohol consumption were predictive of attenuated brain volume abnormalities encourages the inclusion of alcohol recovery efforts in HIV/AIDS therapeutic settings.
Copyright © 2012 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- UNAIDS . Report on the Global HIV/AIDS Epidemic: Executive Summary. UNAIDS; Geneva, Switzerland: 2008.
-
- Goodkin K, Wilkie FL, Concha M, Hinkin CH, Symes S, Baldewicz TT, et al. Aging and neuro-AIDS conditions and the changing spectrum of HIV-1-associated morbidity and mortality. J Clin Epidemiol. 2001;54(Suppl 1):S35–43. - PubMed
-
- Hooshyar D, Hanson DL, Wolfe M, Selik RM, Buskin SE, McNaghten AD. Trends in perimortal conditions and mortality rates among HIV-infected patients. Aids. 2007;21:2093–2100. - PubMed
-
- Gonzalez R, Cherner M. Co-factors in HIV neurobehavioural disturbances: substance abuse, hepatitis C and aging. Int Rev Psychiatry. 2008;20:49–60. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AA005965/AA/NIAAA NIH HHS/United States
- AA017168/AA/NIAAA NIH HHS/United States
- AA005965/AA/NIAAA NIH HHS/United States
- AA017347/AA/NIAAA NIH HHS/United States
- K05 AA017168/AA/NIAAA NIH HHS/United States
- R01 EB008381/EB/NIBIB NIH HHS/United States
- AA010723/AA/NIAAA NIH HHS/United States
- U01 AA017347/AA/NIAAA NIH HHS/United States
- AA012388/AA/NIAAA NIH HHS/United States
- R37 AA005965/AA/NIAAA NIH HHS/United States
- R37 AA010723/AA/NIAAA NIH HHS/United States
- R01 AA017347/AA/NIAAA NIH HHS/United States
- R01 AA012388/AA/NIAAA NIH HHS/United States
- EB008381/EB/NIBIB NIH HHS/United States
- R01 AA010723/AA/NIAAA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
