

Randomized controlled trial of atorvastatin in clinically isolated syndrome: the STAyCIS study
- PMID: 22459680
- PMCID: PMC3320055
- DOI: 10.1212/WNL.0b013e31824f7fdd
Randomized controlled trial of atorvastatin in clinically isolated syndrome: the STAyCIS study
Abstract
Objective: To test efficacy and safety of atorvastatin in subjects with clinically isolated syndrome (CIS).
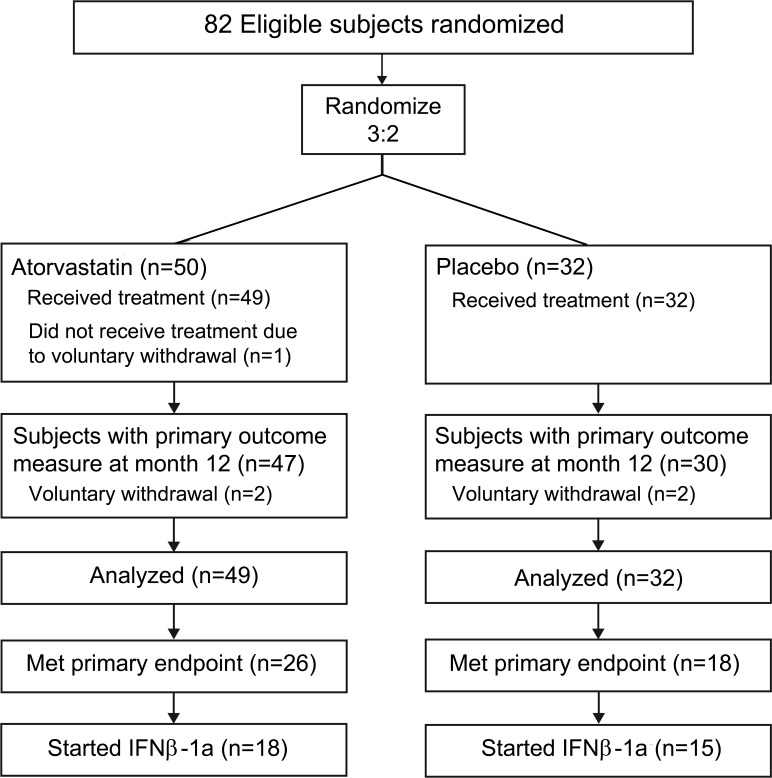
Methods: Subjects with CIS were enrolled in a phase II, double-blind, placebo-controlled, 14-center randomized trial testing 80 mg atorvastatin on clinical and brain MRI activity. Brain MRIs were performed quarterly. The primary endpoint (PEP) was development of ≥ 3 new T2 lesions, or one clinical relapse within 12 months. Subjects meeting the PEP were offered additional weekly interferon β-1a (IFNβ-1a).
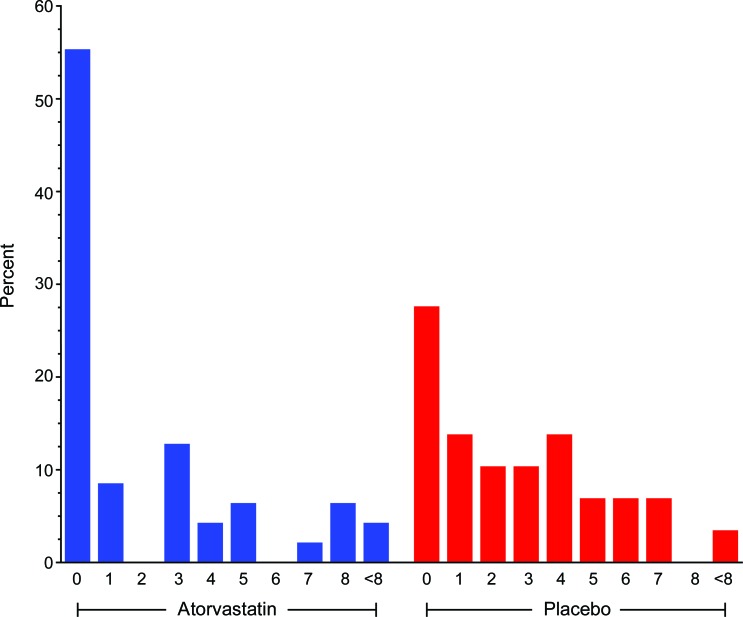
Results: Due to slow recruitment, enrollment was discontinued after 81 of 152 planned subjects with CIS were randomized and initiated study drug. Median (interquartile range) numbers of T2 and gadolinium-enhancing (Gd) lesions were 15.0 (22.0) and 0.0 (0.0) at baseline. A total of 53.1% of atorvastatin recipients (n = 26/49) met PEP compared to 56.3% of placebo recipients (n = 18/32) (p = 0.82). Eleven atorvastatin subjects (22.4%) and 7 placebo subjects (21.9%) met the PEP by clinical criteria. Proportion of subjects who did not develop new T2 lesions up to month 12 or to starting IFNβ-1a was 55.3% in the atorvastatin and 27.6% in the placebo group (p = 0.03). Likelihood of remaining free of new T2 lesions was significantly greater in the atorvastatin group compared with placebo (odds ratio [OR] = 4.34, p = 0.01). Likelihood of remaining free of Gd lesions tended to be higher in the atorvastatin group (OR = 2.72, p = 0.11). Overall, atorvastatin was well tolerated. No clear antagonistic effect of atorvastatin plus IFNβ-1a was observed on MRI measures.
Conclusion: Atorvastatin treatment significantly decreased development of new brain MRI T2 lesion activity, although it did not achieve the composite clinical and imaging PEP.
Classification of evidence: This study provided Class II evidence that atorvastatin did not reduce the proportion of patients with CIS meeting imaging and clinical criteria for starting immunomodulating therapy after 12 months, compared to placebo. In an analysis of a secondary endpoint (Class III), atorvastatin was associated with a reduced risk for developing new T2 lesions.
Figures
References
-
- Zamvil SS, Steinman L. Cholesterol-lowering statins possess anti-inflammatory activity that might be useful for treatment of MS. Neurology 2002; 59: 970– 971 - PubMed
-
- Youssef S, Stuve O, Patarroyo JC, et al. The HMG-CoA reductase inhibitor, atorvastatin, promotes a Th2 bias and reverses paralysis in central nervous system autoimmune disease. Nature 2002; 420: 78– 84 - PubMed
-
- Vollmer T, Key L, Durkalski V, et al. Oral simvastatin treatment in relapsing-remitting multiple sclerosis. Lancet 2004; 363: 1607– 1608 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous