

Alterations of TP53 are associated with a poor outcome for patients with hepatocellular carcinoma: evidence from a systematic review and meta-analysis
- PMID: 22459764
- PMCID: PMC3395767
- DOI: 10.1016/j.ejca.2012.03.001
Alterations of TP53 are associated with a poor outcome for patients with hepatocellular carcinoma: evidence from a systematic review and meta-analysis
Abstract
Background: The prognostic significance of p53 aberration in hepatocellular carcinoma (HCC) remains inconclusive. This systematic review and meta-analysis aimed to provide comprehensive evidence on the association of p53 alterations with recurrence-free survival (RFS) and overall survival (OS) in HCC patients.
Methods: Systematic literature searches were conducted until July 2010. Meta-analysis was performed to estimate prognostic effects of p53 alterations on patient outcomes in HCC. Sensitivity and subgroup analyses were also conducted in the meta-analysis.
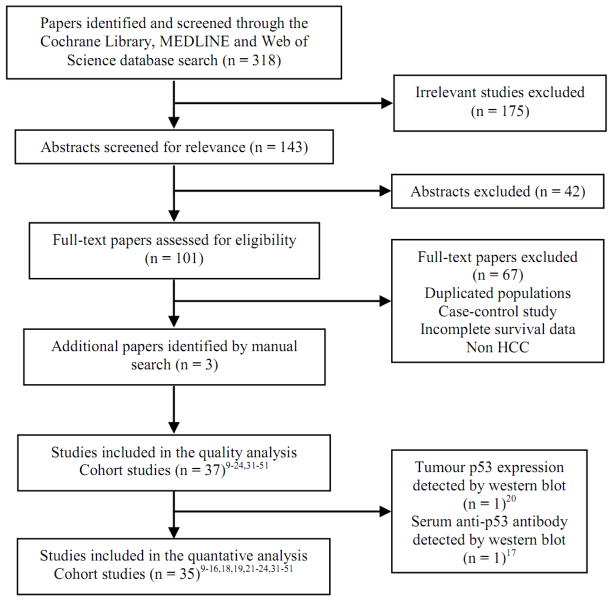
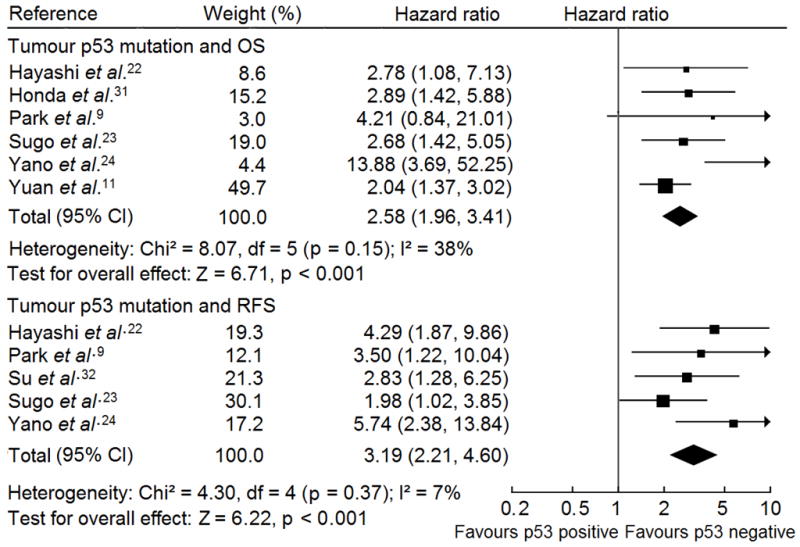
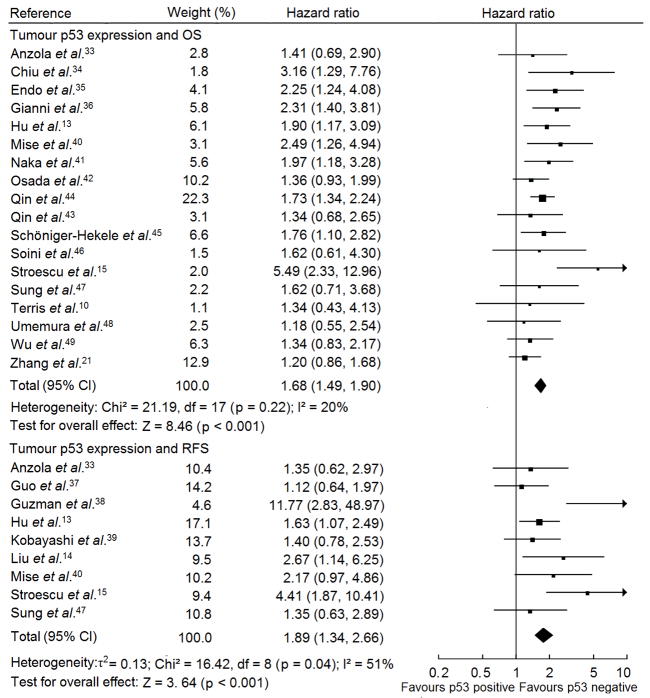
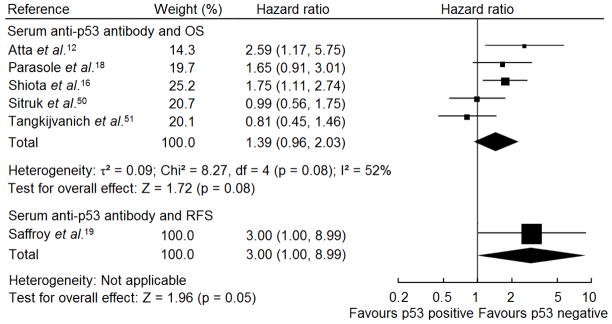
Results: Thirty-seven studies (7 tumour p53 mutation, 23 tumour p53 expression and 7 serum anti-p53 antibodies) were included in the systematic review and meta-analysis. The average percentages of p53 mutation, p53 expression upregulation and anti-p53 antibody level elevation in HCC patients were 31.5%, 35.0% and 23.8%, respectively. Tumour p53 alterations were associated significantly with poor patient outcomes in HCC: the summary hazard ratio (HR) of mutant p53 versus wild type p53 phenotype was 2.58 [95% confidence interval (CI): 1.96-3.41] for OS and 3.19 [95% CI: 2.21-4.60] for RFS, respectively; and the summary HR of upregulated p53 expression versus low/undetectable p53 expression was 1.68 [95% CI: 1.49-1.90] for OS and 1.89 [95% CI: 1.34-2.66] for RFS, respectively. However, elevated serum anti-p53 antibody was only associated with poor OS in HCC group with a high proportion of (≥ 50%) of hepatitis C virus (HCV) infection [HR: 1.92; 95% CI: 1.30-2.85]. Moreover, sensitivity analyses showed that the results of meta-analyses were not altered.
Conclusion: HCC patients with p53 mutation and upregulated expression in tumour tissue have a shorter OS and RFS than patients with wild type p53 and low/undetectable p53 expression. However, the prognostic value of serum anti-p53 antibody is required to be further examined.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors of this manuscript have no potential conflicts of interest to declare.
Figures
References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–917. - PubMed
-
- Jemal A, Siegel RWE, Hao YP, Xu JQ, Thun MJ. Cancer Statistics, 2009. CA Cancer J Clin. 2009;59(4):225–49. - PubMed
-
- McGlynn KA, Tsao L, Hsing AW, Devesa SS, Fraumeni JF., Jr International trends and patterns of primary liver cancer. Int J Cancer. 2001;94(2):290–96. - PubMed
-
- La Vecchia C, Lucchini F, Franceschi S, Negri E, Levi F. Trends in mortality from primary liver cancer in Europe. Eur J Cancer. 2000;36(7):909–15. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
