

Expression of cyclooxygenase-2 (COX-2) in pituitary tumours
- PMID: 22460097
- PMCID: PMC3560830
- DOI: 10.12659/msm.882625
Expression of cyclooxygenase-2 (COX-2) in pituitary tumours
Abstract
Background: Microvessel density in angiogenesis is regarded as a prognostic factor of tumour invasiveness, independent of cell proliferation. In recent studies of pituitary tumours, correlation between the expression of cyclooxygenase-2 (COX-2) and micro-vascularization density and microvessel surface density has been established. We studied the expression of COX-2 in different types of pituitary adenomas to determine the usefulness of COX-2 expression as a prognostic factor of tumour progression or recurrence in patients with hypophyseal tumours.
Material/methods: We retrospectively studied a group of 60 patients of mean age 46.7±17.6 (range, 18 to 85) years who underwent pituitary tumour surgery. Expression of COX-2, as determined by immunohistochemistry, was analyzed in relation to histopathology features of tumour, clinical symptoms, MR imaging and post-operative recurrence/progression of disease.
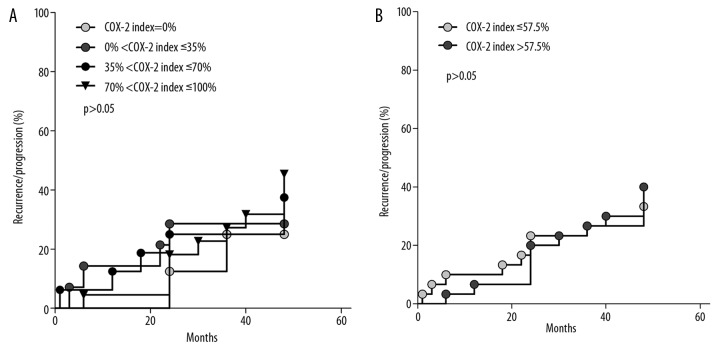
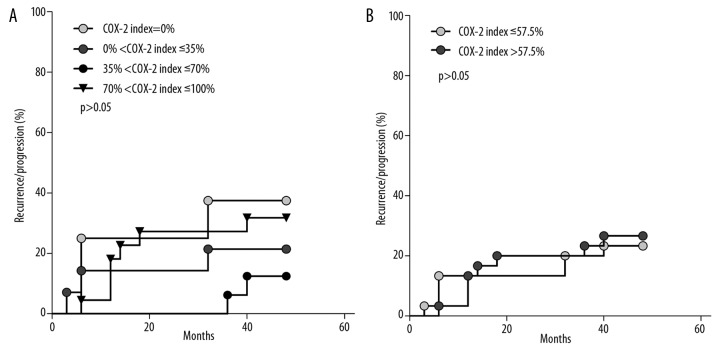
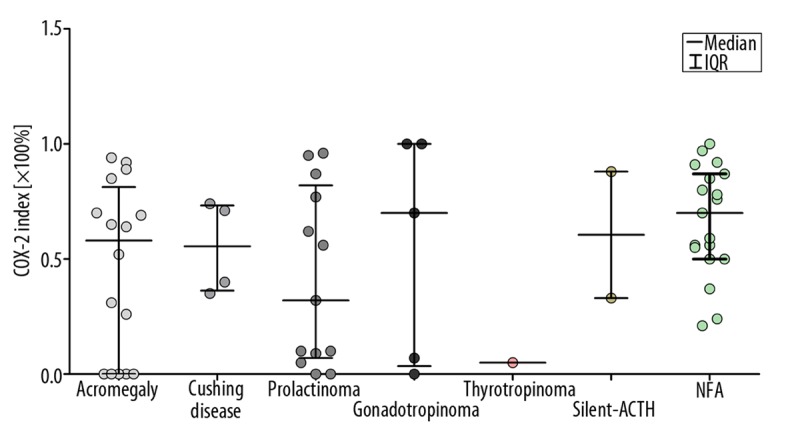
Results: COX-2 was expressed in adenomas of 87% of patients, with a median index value of 57.5% [IQR=60.5]. Highest COX-2 expression was observed in hormonally inactive adenomas and gonadotropinomas and lowest in prolactinomas. We found no differences in COX-2 expression with respect to patient age, gender, tumour size, degree of tumour invasiveness, or whether tumours were immunopositive or immunonegative for pituitary hormones, nor have we found any relation between COX-2 expression and recurrence or progression of tumour size.
Conclusions: COX-2 does not appear to be a predictive factor for recurrence or progression of tumour size. Nevertheless, due to the observed relatively high expression of COX-2 in pituitary adenomas, further studies with COX-2 inhibitors are justified in these tumours.
Figures


References
-
- DeLellis RA, Lloyd RV, Heitz PU, Eng C. Pathology and Genetics of Tumors of Endocrine Organs. 3rd Edition. IARC Press; Lyon: 2004. World Health Organization Classification of Tumors; pp. 9–47.
-
- Dekkers OM, Pereira AM, Roelfsema F, et al. Observation alone after transsphenoidal surgery for nonfunctioning pituitary macroadenoma. J Clin Endocrinol Metab. 2006;91(5):1796–801. - PubMed
-
- Dekkers OM, Pereira AM, Romijn JA. Treatment and follow-up of clinically nonfunctioning pituitary macroadenomas. J Clin Endocrinol Metab. 2008;93(10):3717–26. - PubMed
-
- Colao A, Loche S. Prolactinomas in Children and Adolescents. Endocr Dev. 2010;17:146–59. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
