

Impact of antiretroviral therapy on tuberculosis incidence among HIV-positive patients in high-income countries
- PMID: 22460971
- PMCID: PMC3404691
- DOI: 10.1093/cid/cis203
Impact of antiretroviral therapy on tuberculosis incidence among HIV-positive patients in high-income countries
Abstract
Background: The lower tuberculosis incidence reported in human immunodeficiency virus (HIV)-positive individuals receiving combined antiretroviral therapy (cART) is difficult to interpret causally. Furthermore, the role of unmasking immune reconstitution inflammatory syndrome (IRIS) is unclear. We aim to estimate the effect of cART on tuberculosis incidence in HIV-positive individuals in high-income countries.
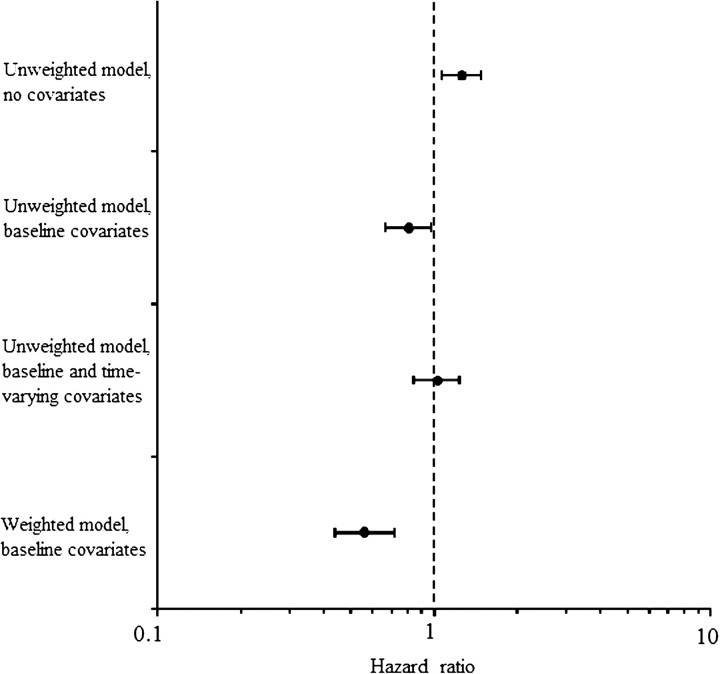
Methods: The HIV-CAUSAL Collaboration consisted of 12 cohorts from the United States and Europe of HIV-positive, ART-naive, AIDS-free individuals aged ≥18 years with baseline CD4 cell count and HIV RNA levels followed up from 1996 through 2007. We estimated hazard ratios (HRs) for cART versus no cART, adjusted for time-varying CD4 cell count and HIV RNA level via inverse probability weighting.
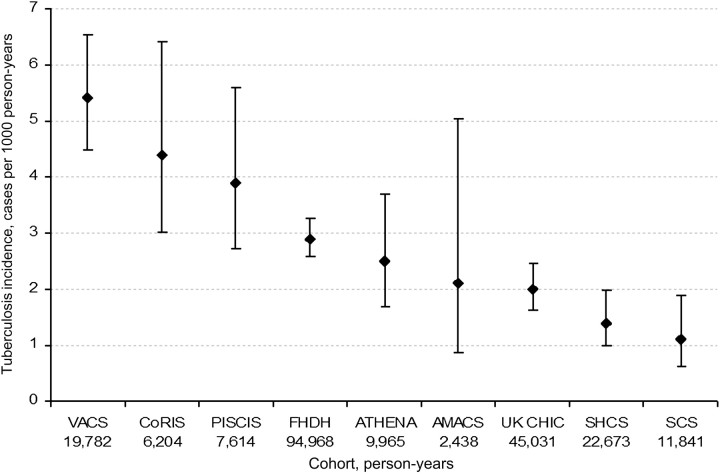
Results: Of 65 121 individuals, 712 developed tuberculosis over 28 months of median follow-up (incidence, 3.0 cases per 1000 person-years). The HR for tuberculosis for cART versus no cART was 0.56 (95% confidence interval [CI], 0.44-0.72) overall, 1.04 (95% CI, 0.64-1.68) for individuals aged >50 years, and 1.46 (95% CI, 0.70-3.04) for people with a CD4 cell count of <50 cells/μL. Compared with people who had not started cART, HRs differed by time since cART initiation: 1.36 (95% CI, 0.98-1.89) for initiation <3 months ago and 0.44 (95% CI, 0.34-0.58) for initiation ≥3 months ago. Compared with people who had not initiated cART, HRs <3 months after cART initiation were 0.67 (95% CI, 0.38-1.18), 1.51 (95% CI, 0.98-2.31), and 3.20 (95% CI, 1.34-7.60) for people <35, 35-50, and >50 years old, respectively, and 2.30 (95% CI, 1.03-5.14) for people with a CD4 cell count of <50 cells/μL.
Conclusions: Tuberculosis incidence decreased after cART initiation but not among people >50 years old or with CD4 cell counts of <50 cells/μL. Despite an overall decrease in tuberculosis incidence, the increased rate during 3 months of ART suggests unmasking IRIS.
Figures
References
-
- Dye C, Watt CJ, Bleed DM, Hosseini SM, Raviglione MC. Evolution of tuberculosis control and prospects for reducing tuberculosis incidence, prevalence, and deaths globally. JAMA. 2005;293:2767–75. - PubMed
-
- STOP TB Partnership. The global plan to stop TB 2006–2015. Available at: http://www.stoptb.org/. Accessed September 2011.
-
- Lawn SD, Wood R, De Cock KM, Kranzer K, Lewis JJ, Churchyard GJ. Antiretrovirals and isoniazid preventive therapy in the prevention of HIV-associated tuberculosis in settings with limited health-care resources. Lancet Infect Dis. 2010;10:489–98. - PubMed
-
- Lawn SD, Bekker LG, Miller RF. Immune reconstitution disease associated with mycobacterial infections in HIV-infected individuals receiving antiretrovirals. Lancet Infect Dis. 2005;5:361–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
