

Detection of infectious influenza virus in cough aerosols generated in a simulated patient examination room
- PMID: 22460981
- PMCID: PMC4680957
- DOI: 10.1093/cid/cis237
Detection of infectious influenza virus in cough aerosols generated in a simulated patient examination room
Abstract
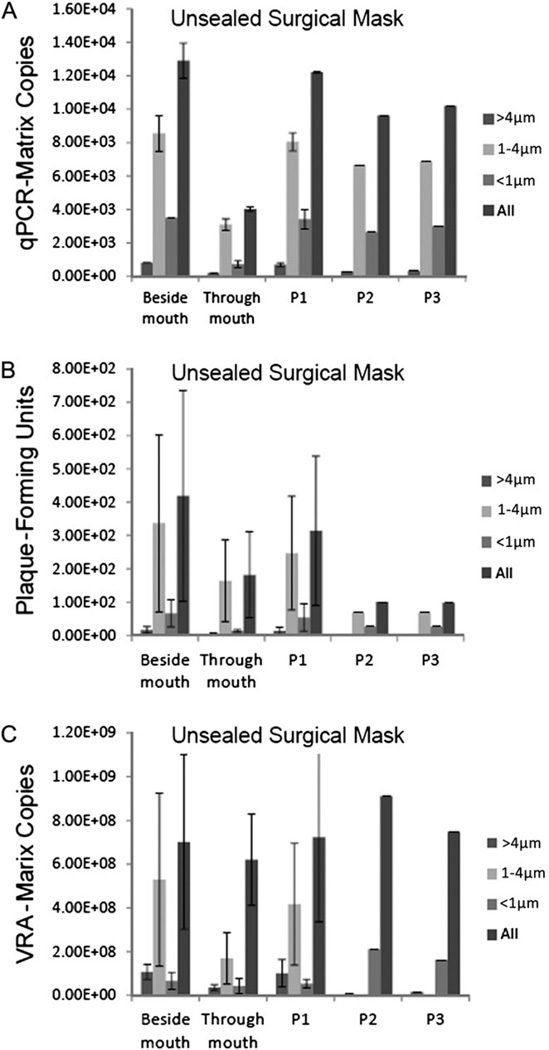
Background: The potential for aerosol transmission of infectious influenza virus (ie, in healthcare facilities) is controversial. We constructed a simulated patient examination room that contained coughing and breathing manikins to determine whether coughed influenza was infectious and assessed the effectiveness of an N95 respirator and surgical mask in blocking transmission.
Methods: National Institute for Occupational Safety and Health aerosol samplers collected size-fractionated aerosols for 60 minutes at the mouth of the breathing manikin, beside the mouth, and at 3 other locations in the room. Total recovered virus was quantitated by quantitative polymerase chain reaction and infectivity was determined by the viral plaque assay and an enhanced infectivity assay.
Results: Infectious influenza was recovered in all aerosol fractions (5.0% in >4 μm aerodynamic diameter, 75.5% in 1-4 μm, and 19.5% in <1 μm; n = 5). Tightly sealing a mask to the face blocked entry of 94.5% of total virus and 94.8% of infectious virus (n = 3). A tightly sealed respirator blocked 99.8% of total virus and 99.6% of infectious virus (n = 3). A poorly fitted respirator blocked 64.5% of total virus and 66.5% of infectious virus (n = 3). A mask documented to be loosely fitting by a PortaCount fit tester, to simulate how masks are worn by healthcare workers, blocked entry of 68.5% of total virus and 56.6% of infectious virus (n = 2).
Conclusions: These results support a role for aerosol transmission and represent the first reported laboratory study of the efficacy of masks and respirators in blocking inhalation of influenza in aerosols. The results indicate that a poorly fitted respirator performs no better than a loosely fitting mask.
Conflict of interest statement
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures





Comment in
-
Airborne transmission of influenza: implications for control in healthcare and community settings.Clin Infect Dis. 2012 Jun;54(11):1578-80. doi: 10.1093/cid/cis240. Epub 2012 Mar 29. Clin Infect Dis. 2012. PMID: 22460979 Free PMC article. No abstract available.
References
-
- IOM (Institute of Medicine) Preventing transmission of pandemic influenza and other viral respiratory diseases: personal protective equipment for healthcare personnel. Washington, DC: National Academies Press; 2011. Update 2010. - PubMed
-
- Wein LM, Atkinson MP. Assessing infection control measures for pandemic influenza. Risk Anal. 2009;29:949–962. - PubMed
-
- Brankston G, Gitterman L, Hirji Z, Lemieux C, Gardam M. Transmission of influenza A in human beings. Lancet Infect Dis. 2007;7:257–265. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
