

Domino Effect: mechanic factors role
- PMID: 22461815
- PMCID: PMC3279072
Domino Effect: mechanic factors role
Abstract
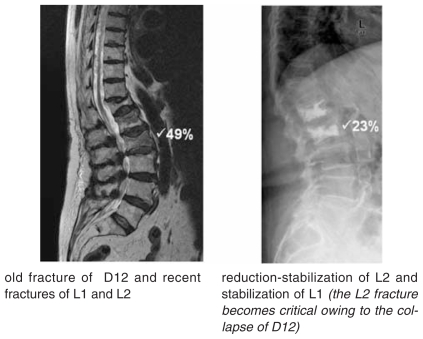
The rapid onset of the Domino Effect following the first Vertebral Compression Fracture is a direct consequence of the mechanical variations that affect the spine when physiological curves are modified. The degree of kyphosis influences the intensity of the Flexor Moment; this is greater on vertebrae D7, D8 and on vertebrae D12, L1 when the spine flexes. Fractures of D7, D8, D12 and L1 are, by far, the most frequent and also the main cause of the mechanical alterations that can trigger the Domino Effect. For these considerations vertebrae D7, D8, D12 and L1 have to be taken in consideration as "critical". In the case of critical clinical vertebral fractures it is useful to provide an indication for minimally invasive surgical reduction or intrasomatic stabilization. When occurs a fracture of a "critical vertebra", prompt restoration of the heights leads to a reduction in the Kyphosis Index and therefore in the Flexor Moment, not only of the fractured vertebra but also, in turn, of all the other metameres which, even if morphologically still intact, are structurally fragile; so, through the restoration of the mechanical vertebral proprieties, we can reduce the risk of the Domino Effect. At the same time the prompt implementation of osteoinductive therapy is indispensable in order to achieve rapid and intense reconstruction of the trabecular bone, the strength of which increases significantly in a short period of time. Clinical studies are necessary to confirm the reduction of the domino effect following a fragility fracture of "critical vertebrae" with the restoration of the mechanical properties together with anabolic therapy.
Keywords: Domino Effect (DE); Flexor Moment (FM); Kyphosis Index (KI); Polymethylmethacrylate (PMMA); Vertebral Compression Fracture (VCF); Vertebral Compression Fractures (VCFs); Vertebral Deformity Degree (VDD); Vertebral Deformity Exacerbation Rate (VDER); Vertebral Deformity Gain (VDG).
Figures







References
-
- Lindsay R, Silverman SL, Cooper C, Hanley DA, Barton I, Broy SB, Licata A, Benhamou L, Geusens P, Flowers K, Stracke H, See-man E. Risk of new vertebral fracture in the year following a fracture. JAMA. 2001 Jan 17;285(3):320–3. - PubMed
-
- Reginster J, Minne HW, Sorensen OH, Hooper M, Roux C, Brandi ML, Lund B, Ethgen D, Pack S, Roumagnac I, Eastell R. Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate therapy (VERT) Study Group. Osteoporos Int. 2000;11(1):83–91. - PubMed
-
- Delmas PD, Genant HK, Crans GG, Stock JL, Wong M, Siris E, Adachi JD. Severity of prevalent vertebral fractures and the risk of subsequent vertebral and nonvertebral fractures: results from the MORE trial. Bone. 2003 Oct;33(4:):522–32. - PubMed
-
- Gallagher, et al. FIT Study. Calcif Tissue Int. 2003
-
- Lunt M, O'Neill TW, Felsenberg D, Reeve J, Kanis JA, Cooper C, Silman AJ European Prospective Osteoporosis Study Group. Characteristics of a prevalent vertebral deformity predict subsequent vertebral fracture: results from the European Prospective Osteoporosis Study (EPOS) Bone. 2003 Oct;33(4):505–13. - PubMed
LinkOut - more resources
Full Text Sources