

Medical evaluation and triage of the agitated patient: consensus statement of the american association for emergency psychiatry project Beta medical evaluation workgroup
- PMID: 22461915
- PMCID: PMC3298208
- DOI: 10.5811/westjem.2011.9.6863
Medical evaluation and triage of the agitated patient: consensus statement of the american association for emergency psychiatry project Beta medical evaluation workgroup
Abstract
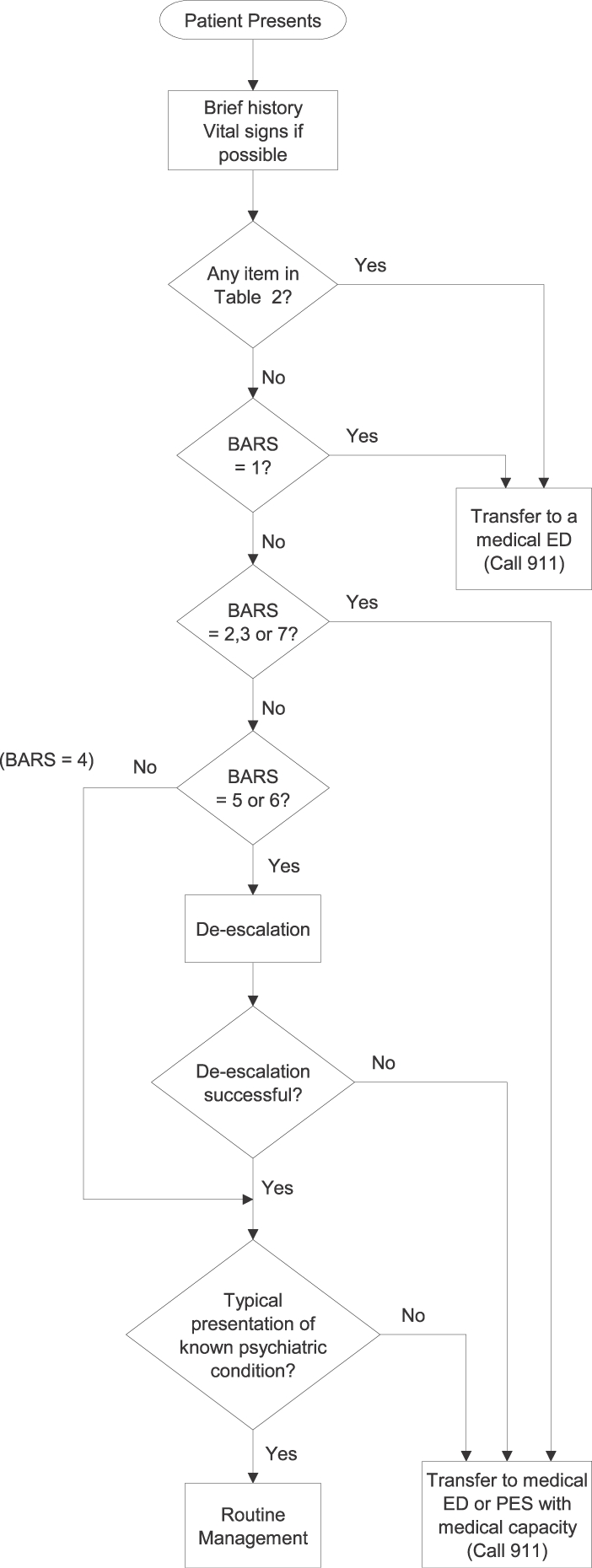
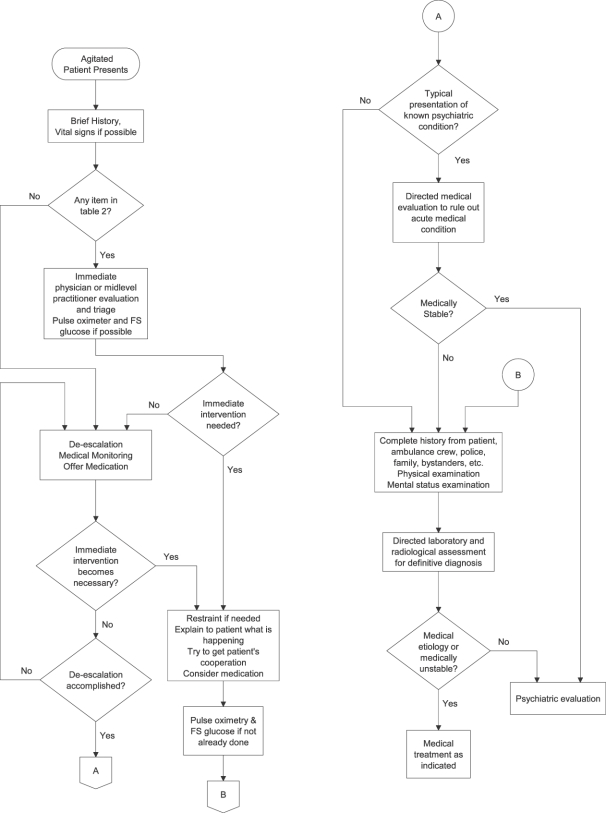
Numerous medical and psychiatric conditions can cause agitation; some of these causes are life threatening. It is important to be able to differentiate between medical and nonmedical causes of agitation so that patients can receive appropriate and timely treatment. This article aims to educate all clinicians in nonmedical settings, such as mental health clinics, and medical settings on the differing levels of severity in agitation, basic triage, use of de-escalation, and factors, symptoms, and signs in determining whether a medical etiology is likely. Lastly, this article focuses on the medical workup of agitation when a medical etiology is suspected or when etiology is unclear.
Conflict of interest statement
Figures
References
-
- Kopecky HJ, Kopecky CR, Yudofsky SC. Reliability and validity of the Overt Agitation Severity Scale in adult psychiatric inpatients. Psychiatr Q. 1998;69:301–323. - PubMed
-
- Silver JM, Yudofsky SC. The Overt Aggression Scale: overview and guiding principles. J Neuropsychiatry Clin Neurosci. 1991;3:S22–S29. - PubMed
-
- Swift RH, Harrigan EP, Cappelleri JC, et al. Validation of the behavioural activity rating scale (BARS): a novel measure of activity in agitated patients. J Psychiatr Res. 2002;36:87–95. - PubMed
-
- Olshaker JS, Browne B, Jerrard DA, et al. Medical clearance and screening of psychiatric patients in the emergency department. Acad Emerg Med. 1997;4:124–128. - PubMed
