

Psychiatric evaluation of the agitated patient: consensus statement of the american association for emergency psychiatry project Beta psychiatric evaluation workgroup
- PMID: 22461916
- PMCID: PMC3298217
- DOI: 10.5811/westjem.2011.9.6868
Psychiatric evaluation of the agitated patient: consensus statement of the american association for emergency psychiatry project Beta psychiatric evaluation workgroup
Abstract
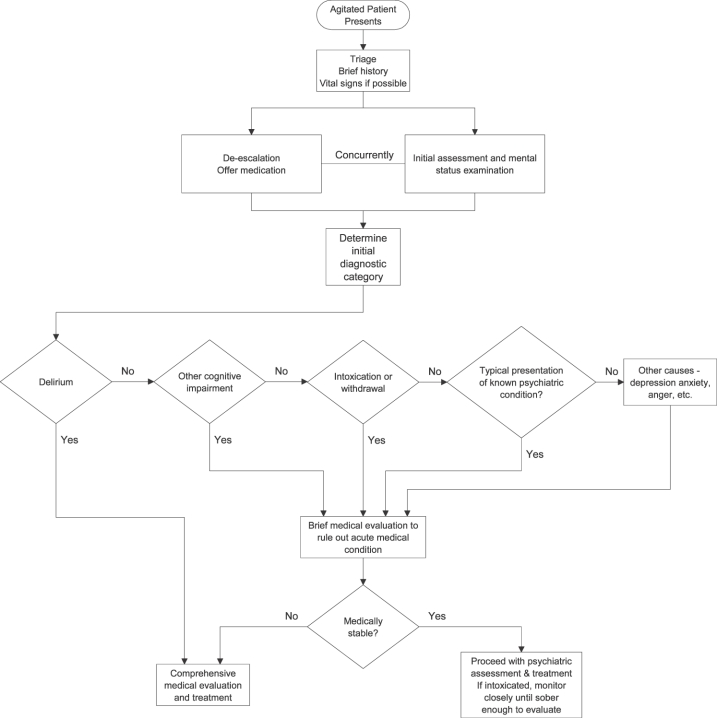
It is difficult to fully assess an agitated patient, and the complete psychiatric evaluation usually cannot be completed until the patient is calm enough to participate in a psychiatric interview. Nonetheless, emergency clinicians must perform an initial mental status screening to begin this process as soon as the agitated patient presents to an emergency setting. For this reason, the psychiatric evaluation of the agitated patient can be thought of as a 2-step process. First, a brief evaluation must be aimed at determining the most likely cause of agitation, so as to guide preliminary interventions to calm the patient. Once the patient is calmed, more extensive psychiatric assessment can be completed. The goal of the emergency assessment of the psychiatric patient is not necessarily to obtain a definitive diagnosis. Rather, ascertaining a differential diagnosis, determining safety, and developing an appropriate treatment and disposition plan are the goals of the assessment. This article will summarize what components of the psychiatric assessment can and should be done at the time the agitated patient presents to the emergency setting. The complete psychiatric evaluation of the patient whose agitation has been treated successfully is beyond the scope of this article and Project BETA (Best practices in Evaluation and Treatment of Agitation), but will be outlined briefly to give the reader an understanding of what a full psychiatric assessment would entail. Other issues related to the assessment of the agitated patient in the emergency setting will also be discussed.
Conflict of interest statement
Figures
Similar articles
-
Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation).J Am Coll Emerg Physicians Open. 2020 Jul 3;1(5):898-907. doi: 10.1002/emp2.12138. eCollection 2020 Oct. J Am Coll Emerg Physicians Open. 2020. PMID: 33145538 Free PMC article. Review.
-
Medical evaluation and triage of the agitated patient: consensus statement of the american association for emergency psychiatry project Beta medical evaluation workgroup.West J Emerg Med. 2012 Feb;13(1):3-10. doi: 10.5811/westjem.2011.9.6863. West J Emerg Med. 2012. PMID: 22461915 Free PMC article.
-
Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup.West J Emerg Med. 2012 Feb;13(1):17-25. doi: 10.5811/westjem.2011.9.6864. West J Emerg Med. 2012. PMID: 22461917 Free PMC article.
-
Best Practices for Evaluation and Treatment of Agitated Children and Adolescents (BETA) in the Emergency Department: Consensus Statement of the American Association for Emergency Psychiatry.Focus (Am Psychiatr Publ). 2023 Jan;21(1):80-88. doi: 10.1176/appi.focus.23022005. Epub 2023 Jan 16. Focus (Am Psychiatr Publ). 2023. PMID: 37205041 Free PMC article.
-
[Acute agitation conditions].Nervenarzt. 2015 Sep;86(9):1111-9. doi: 10.1007/s00115-014-4149-9. Nervenarzt. 2015. PMID: 26173409 Review. German.
Cited by
-
Recognition and management of agitation in acute mental health services: a qualitative evaluation of staff perceptions.BMC Nurs. 2020 Nov 10;19(1):106. doi: 10.1186/s12912-020-00495-x. BMC Nurs. 2020. PMID: 33292208 Free PMC article.
-
Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation).J Am Coll Emerg Physicians Open. 2020 Jul 3;1(5):898-907. doi: 10.1002/emp2.12138. eCollection 2020 Oct. J Am Coll Emerg Physicians Open. 2020. PMID: 33145538 Free PMC article. Review.
-
Clinical and Sociodemographic Profile of Psychomotor Agitation in Mental Health Hospitalisation: A Multicentre Study.Int J Environ Res Public Health. 2022 Nov 30;19(23):15972. doi: 10.3390/ijerph192315972. Int J Environ Res Public Health. 2022. PMID: 36498042 Free PMC article.
-
Interventions to prevent aggression against doctors: a systematic review.BMJ Open. 2019 Sep 17;9(9):e028465. doi: 10.1136/bmjopen-2018-028465. BMJ Open. 2019. PMID: 31530592 Free PMC article.
-
Updates in the Assessment and Management of Agitation.Focus (Am Psychiatr Publ). 2023 Jan;21(1):35-45. doi: 10.1176/appi.focus.20220064. Epub 2023 Jan 16. Focus (Am Psychiatr Publ). 2023. PMID: 37205032 Free PMC article.
