

Use and avoidance of seclusion and restraint: consensus statement of the american association for emergency psychiatry project Beta seclusion and restraint workgroup
- PMID: 22461919
- PMCID: PMC3298214
- DOI: 10.5811/westjem.2011.9.6867
Use and avoidance of seclusion and restraint: consensus statement of the american association for emergency psychiatry project Beta seclusion and restraint workgroup
Abstract
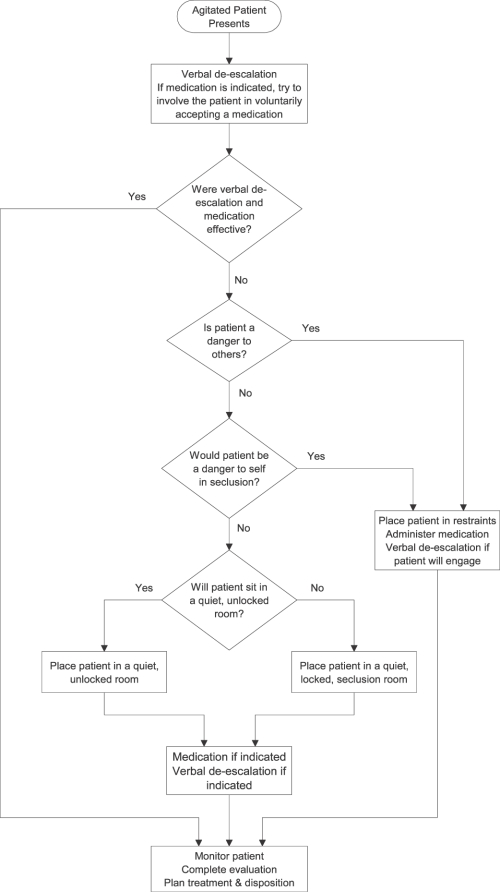
Issues surrounding reduction and/or elimination of episodes of seclusion and restraint for patients with behavioral problems in crisis clinics, emergency departments, inpatient psychiatric units, and specialized psychiatric emergency services continue to be an area of concern and debate among mental health clinicians. An important underlying principle of Project BETA (Best practices in Evaluation and Treatment of Agitation) is noncoercive de-escalation as the intervention of choice in the management of acute agitation and threatening behavior. In this article, the authors discuss several aspects of seclusion and restraint, including review of the Centers for Medicare and Medicaid Services guidelines regulating their use in medical behavioral settings, negative consequences of this intervention to patients and staff, and a review of quality improvement and risk management strategies that have been effective in decreasing their use in various treatment settings. An algorithm designed to help the clinician determine when seclusion or restraint is most appropriate is introduced. The authors conclude that the specialized psychiatric emergency services and emergency departments, because of their treatment primarily of acute patients, may not be able to entirely eliminate the use of seclusion and restraint events, but these programs can adopt strategies to reduce the utilization rate of these interventions.
Conflict of interest statement
Figures
References
-
- Department of Health and Human Services. Condition of participation: patient's rights. Federal Register 482.13. 2006. pp. 71426–71428.
-
- Haimowitz S, Urff J, Huckshorn KA. Restraint and seclusion—a risk management guide. 2011. National Association of State Mental Health Program Directors Web site. Available at: http://www.nasmhpd.org/general_files/publications/ntac_pubs/R-S RISK MGMT 10-10-06.pdf. Accessed July 6.
-
- Fisher WA. Restraint and seclusion: a review of the literature. Am J Psychiatry. 1994;151:1584–1591. - PubMed
-
- Mohr WK, Petti TA, Mohr BD. Adverse effects associated with physical restraint. Can J Psychiatry. 2003;48:330–337. - PubMed
