

Dose-dependent response to cyclodextrin infusion in a rat model of verapamil toxicity
- PMID: 22461924
- PMCID: PMC3298207
- DOI: 10.5811/westjem.2011.3.6696
Dose-dependent response to cyclodextrin infusion in a rat model of verapamil toxicity
Abstract
Introduction: Sulfobutylether-β-cyclodextrin (SBE-CD) is a pharmaceutical excipient known to bind verapamil. Following intravenous administration, clearance of SBE-CD approximates glomerular filtration rate. We hypothesized that infusion of SBE-CD would increase time to asystole in a rat model of verapamil toxicity in a dose-dependent manner. The objective was to demonstrate the effect of a range of SBE-CD concentrations in a rat model of verapamil toxicity.
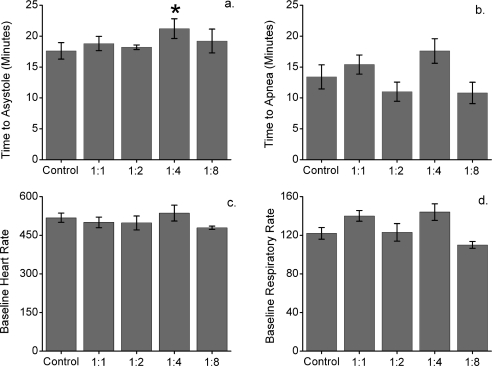
Methods: Twenty-five Wistar rats were allocated to control or 1 of 4 intervention groups. All received ketamine and diazepam anesthesia followed by verapamil infusion 32 mg/kg/h. The verapamil infusion for the intervention groups was premixed with SBE-CD in a 1:1, 1:2, 1:4, or 1:8 molar ratio (verapamil to SBE-CD). The control group infusion did not contain SBE-CD. Additional saline or water was added to the infusion so that the total volume infused was the same across groups, and the osmolality was maintained as close to physiologic as possible. Heart rate, respiratory rate, and temperature were monitored. The primary endpoint was time to asystole.
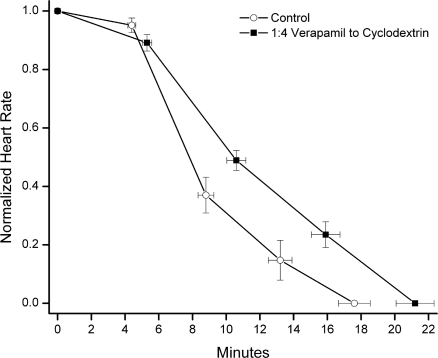
Results: Verapamil coinfused with SBE-CD in a molar ratio of 1:4 resulted in prolonged time to asystole compared to control (21.2 minutes vs 17.6 minutes, P < 0.05). There were no differences in time to asystole between control and any other intervention group. There was no significant difference in time to apnea between control and any intervention group. We assessed the effect of a range of SBE-CD concentrations and identified 1 concentration that prolonged time to asystole. Mechanisms that may explain this effect include optimal volume expansion with a hyperosmolar cyclodextrin containing solution, complexation of verapamil within the hydrophobic cyclodextrin pore, and/or complexation within micelle-like aggregates of cyclodextrin. However, mechanistic explanations for the observed findings are speculative at this point.
Conclusion: The 1:4 verapamil to SBE-CD concentration was modestly effective with SBE-CD concentrations above and below this range demonstrating nonstatistically significant improvements in time to asystole.
Conflict of interest statement
Figures
References
-
- Bom A, Bradley M, Cameron K, et al. A novel concept of reversing neuromuscular block: chemical encapsulation of rocuronium bromide by a cyclodextrin-based synthetic host. Angew Chem Int Ed Engl. 2002;41:266–270. - PubMed
-
- Sparr HJ, Vermeyen KM, Beaufort AM, et al. Early reversal of profound rocuronium-induced neuromuscular blockade by sugammadex in a randomized multicenter study: efficacy, safety, and pharmacokinetics. Anesthesiology. 2007;106:935–943. - PubMed
-
- Szejtli J. Comprehensive Supramolecular Chemistry. New York, NY: Elsevier;; 1996.
-
- Loftsson T, Magnusdottir A, Masson M, et al. Self-association and cyclodextrin solubilization of drugs. J Pharm Sci. 2002;91:2307–2316. - PubMed
