

Effect of large incisor retraction on upper airway morphology in adult bimaxillary protrusion patients
- PMID: 22462464
- PMCID: PMC8813144
- DOI: 10.2319/110211-675.1
Effect of large incisor retraction on upper airway morphology in adult bimaxillary protrusion patients
Abstract
Objective: To evaluate, using multislice computed tomography (MSCT), the morphologic changes in the upper airway after large incisor retraction in adult bimaxillary protrusion patients.
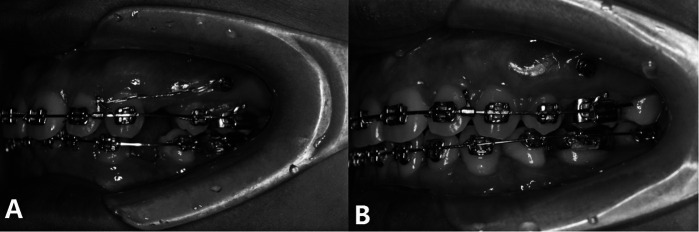
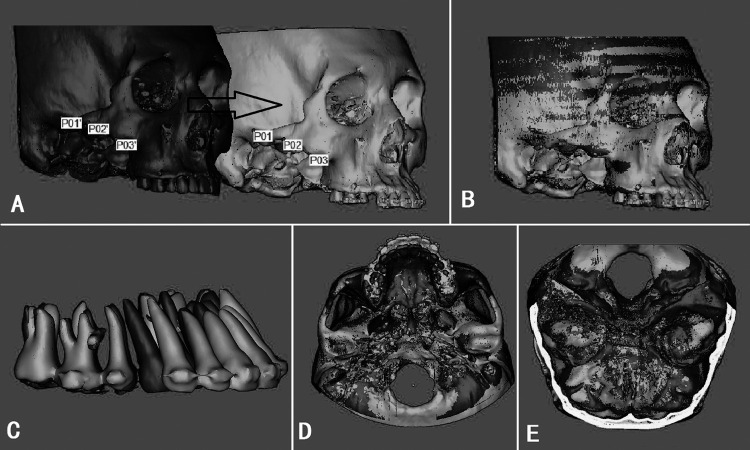
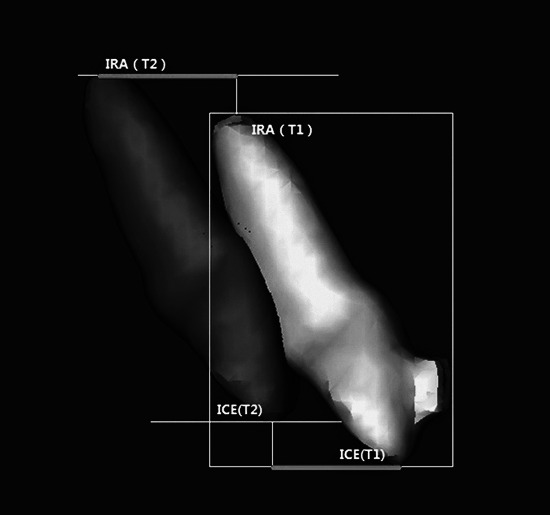
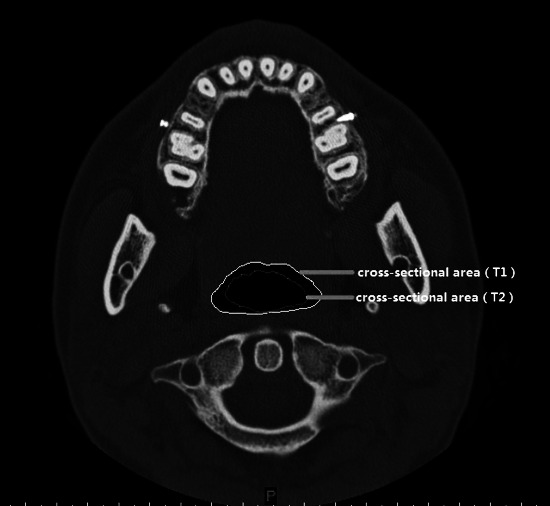
Materials and methods: Thirty adult patients with bimaxillary protrusion had four first premolars extracted, and then miniscrews were placed to provide anchorage. A CT scan was performed before incisor retraction and again posttreatment. Three-dimensional (3D) reconstruction of the pre- (T1) and post- (T2) CT data was used to assess for morphological changes of the upper airway. A paired t-test was used to compare changes from T1 to T2. The relationship among the three variables (upper incisor retraction amount, upper airway size, and hyoid position) was analyzed by Pearson correlation coefficient.
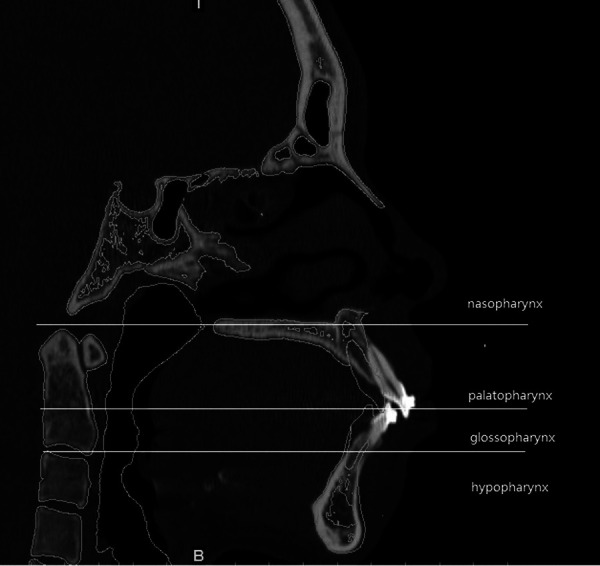
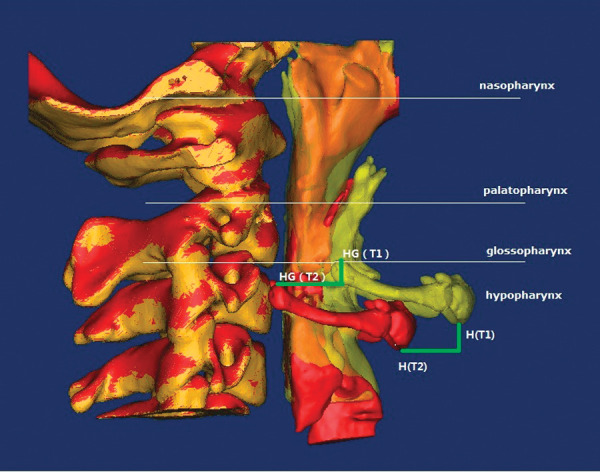
Results: The amounts of upper incisor retraction at the incisal edge and apex were 7.64 ± 1.68 mm and 3.91 ± 2.10 mm, respectively. The hyoid was retracted 2.96 ± 0.54 mm and 9.87 ± 2.92 mm, respectively, in the horizontal and vertical directions. No significant difference was observed in the mean cross-sectional area of the nasopharynx (P > .05) between T1 and T2, while significant differences between T1 and T2 were found in the mean cross-sectional areas of the palatopharynx, glossopharynx, and hypopharynx (P < .05); these mean cross-sectional areas were decreased by 21.02% ± 7.89%, 25.18% ± 13.51%, and 38.19% ± 5.51%, respectively. The largest change in the cross-sectional area is always noted in the hypopharynx. There was a significant correlation among the retraction distance of the upper incisor at its edge, the retraction distance of the hyoid in the horizontal direction, and the decrease of the hypopharynx.
Conclusion: Large incisor retraction leads to narrowing of the upper airway in adult bimaxillary protrusion patients.
Figures
References
-
- Bills D. A, Handelman C. S, BeGole E. A. Bimaxillary dentoalveolar protrusion: traits and orthodontic correction. Angle Orthod. 2005;75:333–339. - PubMed
-
- Lai E. H, Yao C. C, Chang J. Z, Chen I, Chen Y. J. Three-dimensional dental model analysis of treatment outcomes for protrusive maxillary dentition: comparison of headgear, miniscrew, and miniplate skeletal anchorage. Am J Orthod Dentofacial Orthop. 2008;134:636–645. - PubMed
-
- Yao C. C, Lai E. H, Chang J. Z, Chen I, Chen Y. J. Comparison of treatment outcomes between skeletal anchorage and extraoral anchorage in adults with maxillary dentoalveolar protrusion. Am J Orthod Dentofacial Orthop. 2008;134:615–624. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
