

GFR at initiation of dialysis and mortality in CKD: a meta-analysis
- PMID: 22465328
- PMCID: PMC3395227
- DOI: 10.1053/j.ajkd.2012.01.015
GFR at initiation of dialysis and mortality in CKD: a meta-analysis
Abstract
Background: The proportion of patients with advanced chronic kidney disease (CKD) initiating dialysis therapy at a higher glomerular filtration rate (GFR) has increased during the past decade. Recent data suggest that higher GFR may be associated with increased mortality.
Study design: A meta-analysis of cohort studies and trials.
Setting & population: Patients with advanced CKD.
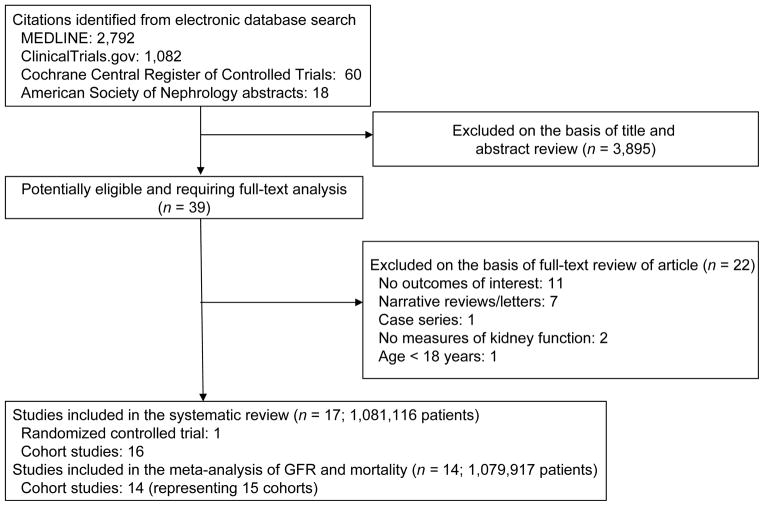
Selection criteria for studies: We performed a systematic literature search in MEDLINE, Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, American Society of Nephrology abstracts, and bibliographies of retrieved articles to identify studies reporting on GFR at dialysis therapy initiation and mortality.
Predictor: Estimated or calculated GFR at dialysis therapy initiation.
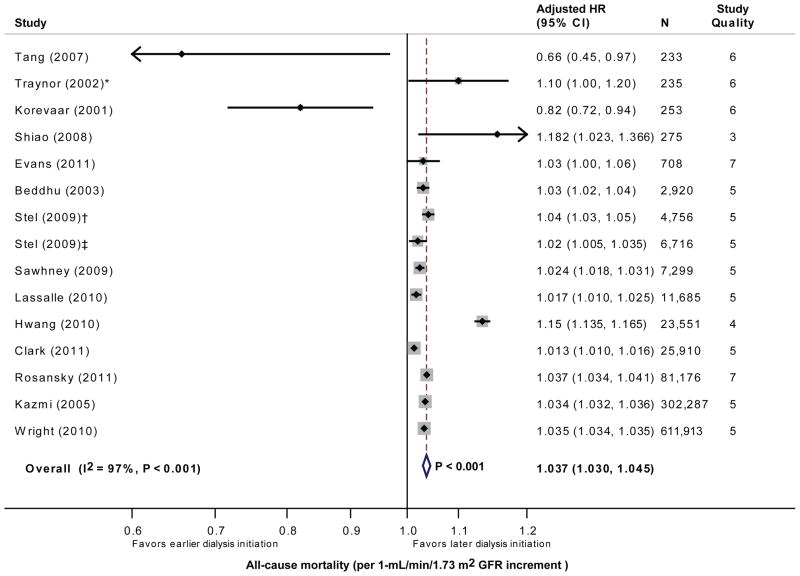
Outcome: Pooled adjusted hazard ratio (HR) of continuous GFR for all-cause mortality.
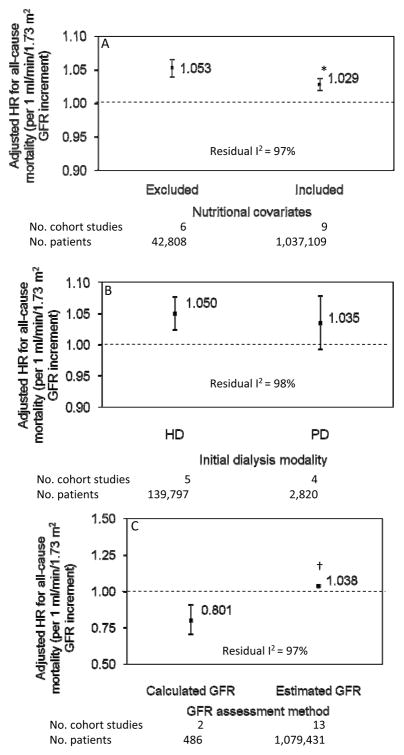
Results: 16 cohort studies and 1 randomized controlled trial were identified (n = 1,081,116). By meta-analysis restricted to 15 cohorts (n = 1,079,917), higher GFR at dialysis therapy initiation was associated with a higher pooled adjusted HR for all-cause mortality (1.04; 95% CI, 1.03-1.05; P < 0.001). However, there was significant heterogeneity (I(2) = 97%; P < 0.001). The association persisted among the 9 cohorts that adjusted analytically for nutritional covariates (HR, 1.03; 95% CI, 1.02-1.04; P < 0.001; residual I(2) = 97%). The highest mortality risk was observed in hemodialysis cohorts (HR, 1.05; 95% CI, 1.02-1.08; P < 0.001), whereas there was no association between GFR and mortality in peritoneal dialysis cohorts (HR, 1.04; 95% CI, 0.99-1.08, P = 0.1; residual I(2) = 98%). Finally, higher GFR was associated with a lower mortality risk in cohorts that calculated GFR (HR, 0.80; 95% CI, 0.71-0.91; P = 0.003), contrasting with a higher mortality risk in cohorts that estimated GFR (HR, 1.04; 95% CI, 1.03-1.05; P < 0.001; residual I(2) = 97%).
Limitations: Paucity of randomized controlled trials, different methods for determining GFR, and substantial heterogeneity.
Conclusions: Higher estimated rather than calculated GFR at dialysis therapy initiation is associated with a higher mortality risk in patients with advanced CKD, independent of nutritional status. Although there was substantial heterogeneity of effect size estimates across studies, this observation requires further study.
Copyright © 2012 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Couchoud C, Stengel B, Landais P, et al. The renal epidemiology and information network (REIN): a new registry for end-stage renal disease in France. Nephrol Dial Transplant. 2006 Feb;21(2):411–418. - PubMed
-
- Klebe B, Irving J, Stevens PE, et al. The cost of implementing UK guidelines for the management of chronic kidney disease. Nephrol Dial Transplant. 2007 Sep;22(9):2504–2512. - PubMed
-
- Collins AJ, Foley R, Herzog C, et al. Excerpts from the United States Renal Data System 2007 annual data report. Am J Kidney Dis. 2008 Jan;51(1 Suppl 1):S1–320. - PubMed
-
- Collins AJ, Foley RN, Herzog C, et al. US Renal Data System 2010 Annual Data Report. Am J Kidney Dis. 2011 Jan;57(1 Suppl 1):A8, e1–526. - PubMed
-
- Stel VS, Tomson C, Ansell D, et al. Level of renal function in patients starting dialysis: an ERA-EDTA Registry study. Nephrol Dial Transplant. 2010 Oct;25(10):3315–3325. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
