

Inspiratory muscle strength training in infants with congenital heart disease and prolonged mechanical ventilation: a case report
- PMID: 22466028
- PMCID: PMC3563028
- DOI: 10.2522/ptj.20110348
Inspiratory muscle strength training in infants with congenital heart disease and prolonged mechanical ventilation: a case report
Abstract
Background and purpose: Inspiratory muscle strength training (IMST) has been shown to improve maximal pressures and facilitate ventilator weaning in adults with prolonged mechanical ventilation (MV). The purposes of this case report are: (1) to describe the rationale for IMST in infants with MV dependence and (2) to summarize the device modifications used to administer training.
Case description: Two infants with congenital heart disease underwent corrective surgery and were referred for inspiratory muscle strength evaluation after repeated weaning failures. It was determined that IMST was indicated due to inspiratory muscle weakness and a rapid, shallow breathing pattern. In order to accommodate small tidal volumes of infants, 2 alternative training modes were devised. For infant 1, IMST consisted of 15-second inspiratory occlusions. Infant 2 received 10-breath sets of IMST through a modified positive end-expiratory pressure valve. Four daily IMST sets separated by 3 to 5 minutes of rest were administered 5 to 6 days per week. The infants' IMST tolerance was evaluated by vital signs and daily clinical reviews.
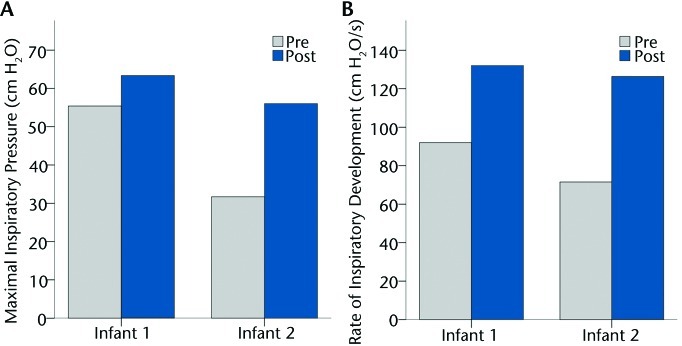
Outcomes: Maximal inspiratory pressure (MIP) and rate of pressure development (dP/dt) were the primary outcome measures. Secondary outcome measures included the resting breathing pattern and MV weaning. There were no adverse events associated with IMST. Infants generated training pressures through the adapted devices, with improved MIP, dP/dt, and breathing pattern. Both infants weaned from MV to a high-flow nasal cannula, and neither required subsequent reintubation during their hospitalization.
Discussion: This case report describes pediatric adaptations of an IMST technique used to improve muscle performance and facilitate weaning in adults. Training was well tolerated in 2 infants with postoperative weaning difficulty and inspiratory muscle dysfunction. Further systematic examination will be needed to determine whether IMST provides a significant performance or weaning benefit.
Figures


References
-
- Levine S, Nguyen T, Taylor N, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med. 2008;358:1327–1335 - PubMed
-
- Gayan-Ramirez G, Testelmans D, Maes K, et al. Intermittent spontaneous breathing protects the rat diaphragm from mechanical ventilation effects. Crit Care Med. 2005;33:2804–2809 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
