

Plus disease in retinopathy of prematurity: diagnostic impact of field of view
- PMID: 22466473
- PMCID: PMC3637840
- DOI: 10.1097/IAE.0b013e31823ac3c3
Plus disease in retinopathy of prematurity: diagnostic impact of field of view
Abstract
Purpose: To examine the impact of retinal field of view and magnification on interexpert reliability of plus disease diagnosis in retinopathy of prematurity.
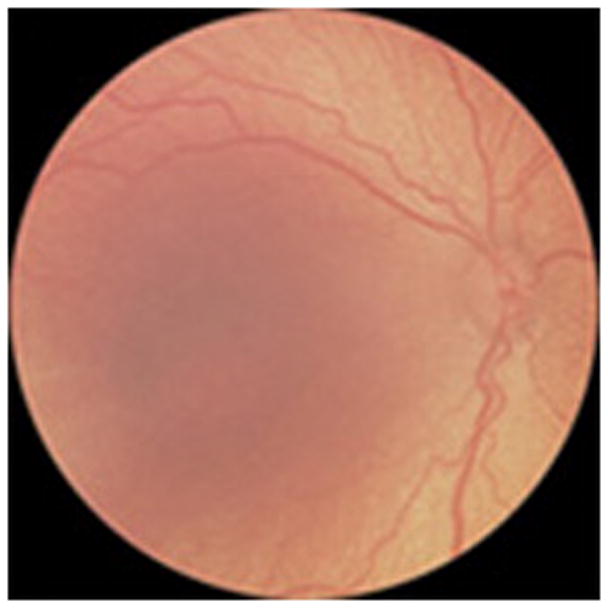
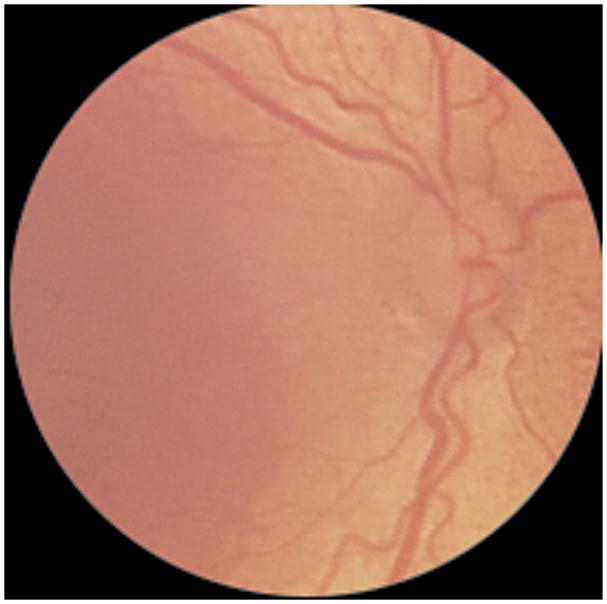
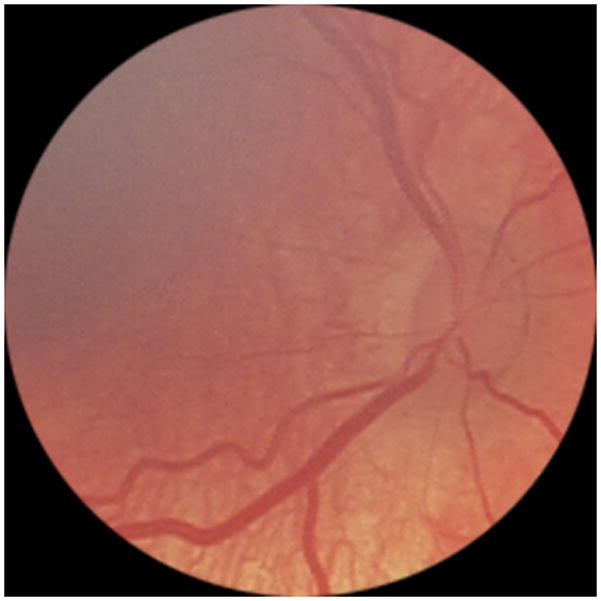
Methods: Fifteen wide-angle images from infants with retinopathy of prematurity were cropped and adjusted in magnification to create 2 additional image categories: medium angle (40°-50°) and narrow angle (20°-30°). These 45 images were uploaded to a Web-based system and interpreted independently by 13 experts of retinopathy of prematurity using a 3-level (plus, preplus, neither) and 2-level (plus, not plus) classification. Absolute agreement and kappa statistics were calculated to compare interexpert reliability.
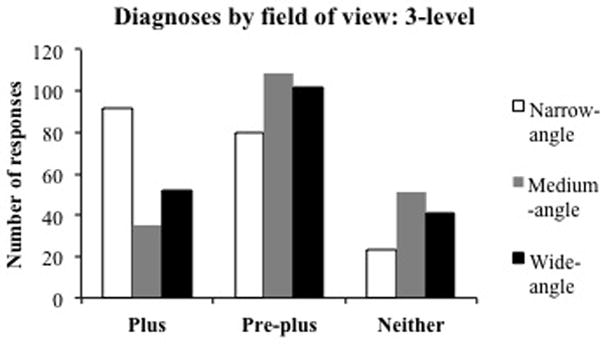
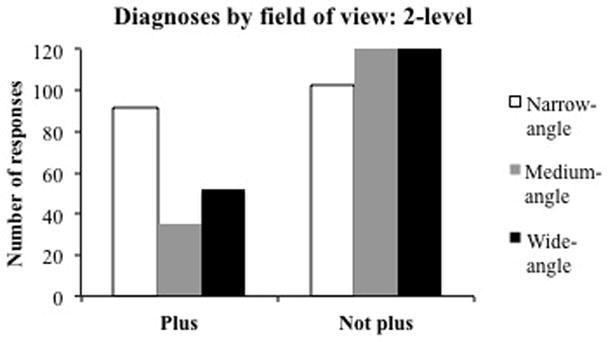
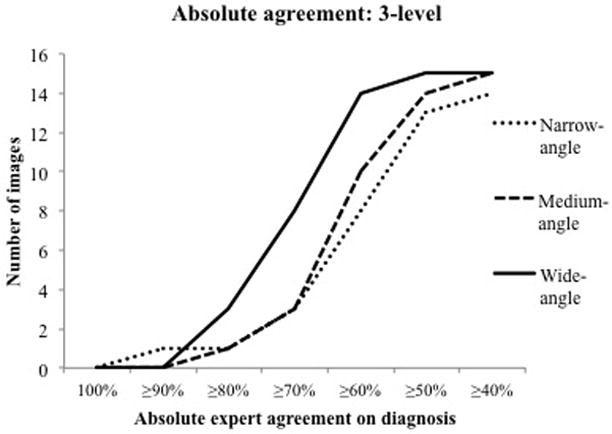
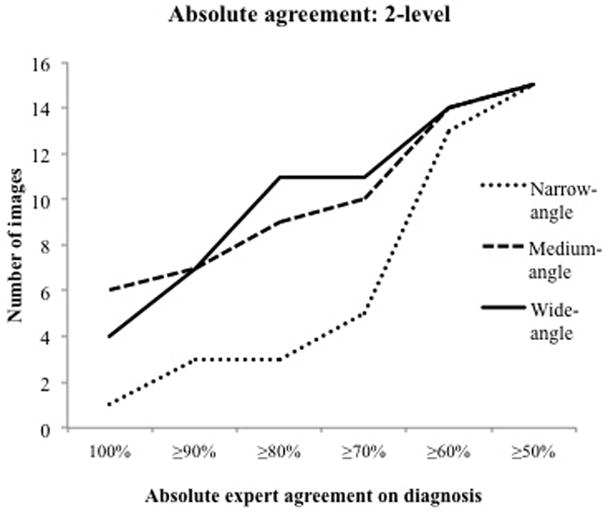
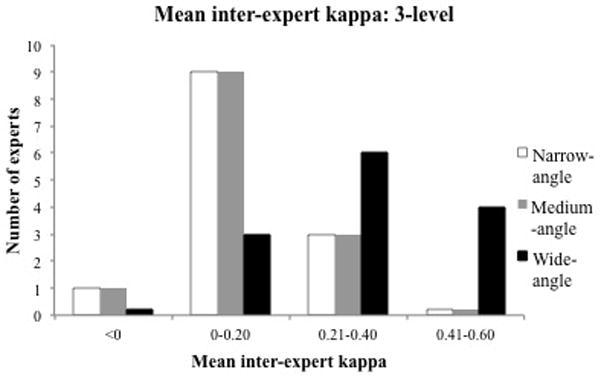
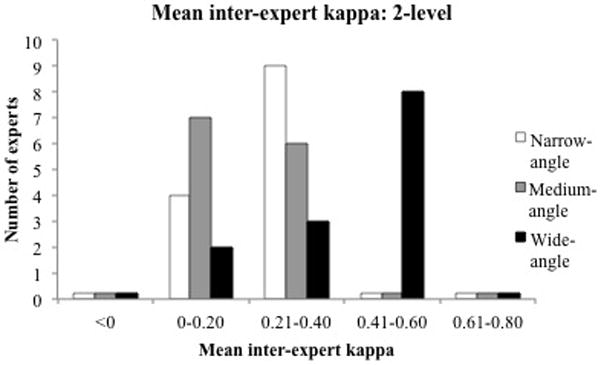
Results: In the 3-level classification, ≥ 70% experts agreed on the same diagnosis in 8 of the 15 wide-angle images (53%), but only in 3 of the 15 medium-angle (20%) and 3 of the 15 narrow-angle (20%) images. In the 2-level classification, ≥ 80% experts agreed on the same diagnosis in 11 of the 15 wide-angle images (73%), but only in 9 of the 15 medium-angle (60%) and 3 of the 15 narrow-angle (20%) images. Mean kappa of each expert compared with all other experts was 0.40 to 0.59 in 8 of 13 experts (62%) using wide-angle images, was 0 to 0.19 in 7 of 13 experts (54%) using medium-angle images, and was 0.20 to 0.39 in 9 of 13 experts (69%) using narrow-angle images.
Conclusion: Interexpert agreement in plus disease diagnosis in wide-angle images is higher than from medium-angle and narrow-angle images. Plus disease is defined using a narrow-angle standard published photograph, yet this study suggests that peripheral findings also contribute to diagnosis.
Conflict of interest statement
No authors have financial conflicts of interest. MFC is an unpaid member of the Scientific Advisory Board for Clarity Medical Systems (Pleasanton, CA).
Figures


Similar articles
-
Interexpert agreement of plus disease diagnosis in retinopathy of prematurity.Arch Ophthalmol. 2007 Jul;125(7):875-80. doi: 10.1001/archopht.125.7.875. Arch Ophthalmol. 2007. PMID: 17620564
-
Plus disease in retinopathy of prematurity: qualitative analysis of diagnostic process by experts.JAMA Ophthalmol. 2013 Aug;131(8):1026-32. doi: 10.1001/jamaophthalmol.2013.135. JAMA Ophthalmol. 2013. PMID: 23702696 Free PMC article.
-
Plus Disease in Retinopathy of Prematurity: A Continuous Spectrum of Vascular Abnormality as a Basis of Diagnostic Variability.Ophthalmology. 2016 Nov;123(11):2338-2344. doi: 10.1016/j.ophtha.2016.07.026. Epub 2016 Aug 31. Ophthalmology. 2016. PMID: 27591053 Free PMC article.
-
Image analysis for retinopathy of prematurity diagnosis.J AAPOS. 2009 Oct;13(5):438-45. doi: 10.1016/j.jaapos.2009.08.011. J AAPOS. 2009. PMID: 19840720 Free PMC article. Review.
-
Plus Disease in Retinopathy of Prematurity: More Than Meets the ICROP?Asia Pac J Ophthalmol (Phila). 2018 May-Jun;7(3):152-155. doi: 10.22608/APO.201863. Epub 2018 May 24. Asia Pac J Ophthalmol (Phila). 2018. PMID: 29797825 Free PMC article. Review.
Cited by
-
Expert Diagnosis of Plus Disease in Retinopathy of Prematurity From Computer-Based Image Analysis.JAMA Ophthalmol. 2016 Jun 1;134(6):651-7. doi: 10.1001/jamaophthalmol.2016.0611. JAMA Ophthalmol. 2016. PMID: 27077667 Free PMC article.
-
Auto-Processed Retinal Vessel Shadow View Images From Bedside Optical Coherence Tomography to Evaluate Plus Disease in Retinopathy of Prematurity.Transl Vis Sci Technol. 2020 Aug 7;9(9):16. doi: 10.1167/tvst.9.9.16. eCollection 2020 Aug. Transl Vis Sci Technol. 2020. PMID: 32879772 Free PMC article.
-
Accuracy and Reliability of Eye-Based vs Quadrant-Based Diagnosis of Plus Disease in Retinopathy of Prematurity.JAMA Ophthalmol. 2018 Jun 1;136(6):648-655. doi: 10.1001/jamaophthalmol.2018.1195. JAMA Ophthalmol. 2018. PMID: 29710185 Free PMC article.
-
Computer-Based Image Analysis for Plus Disease Diagnosis in Retinopathy of Prematurity: Performance of the "i-ROP" System and Image Features Associated With Expert Diagnosis.Transl Vis Sci Technol. 2015 Nov 30;4(6):5. doi: 10.1167/tvst.4.6.5. eCollection 2015 Nov. Transl Vis Sci Technol. 2015. PMID: 26644965 Free PMC article.
-
Influence of Computer-Generated Mosaic Photographs on Retinopathy of Prematurity Diagnosis and Management.JAMA Ophthalmol. 2016 Nov 1;134(11):1283-1289. doi: 10.1001/jamaophthalmol.2016.3625. JAMA Ophthalmol. 2016. PMID: 27685535 Free PMC article.
References
-
- Multicenter trial of cryotherapy for retinopathy of prematurity. Preliminary results. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Arch Ophthalmol. 1988;106:471–9. - PubMed
-
- Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Early Treatment For Retinopathy Of Prematurity Cooperative Group. Arch Ophthalmol. 2003;121:1684–94. - PubMed
-
- An international classification of retinopathy of prematurity. The Committee for the Classification of Retinopathy of Prematurity. Arch Ophthalmol. 1984;102:1130–4. - PubMed
-
- The International Classification of Retinopathy of Prematurity revisited. Arch Ophthalmol. 2005;123:991–9. - PubMed
-
- Chiang MF, Jiang L, Gelman R, Du YE, Flynn JT. Interexpert agreement of plus disease diagnosis in retinopathy of prematurity. Arch Ophthalmol. 2007;125:875–80. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
