

Hepatic artery pseudoaneurysm after endoscopic biliary stenting for bile duct cancer
- PMID: 22468193
- PMCID: PMC3314928
- DOI: 10.4329/wjr.v4.i3.115
Hepatic artery pseudoaneurysm after endoscopic biliary stenting for bile duct cancer
Abstract
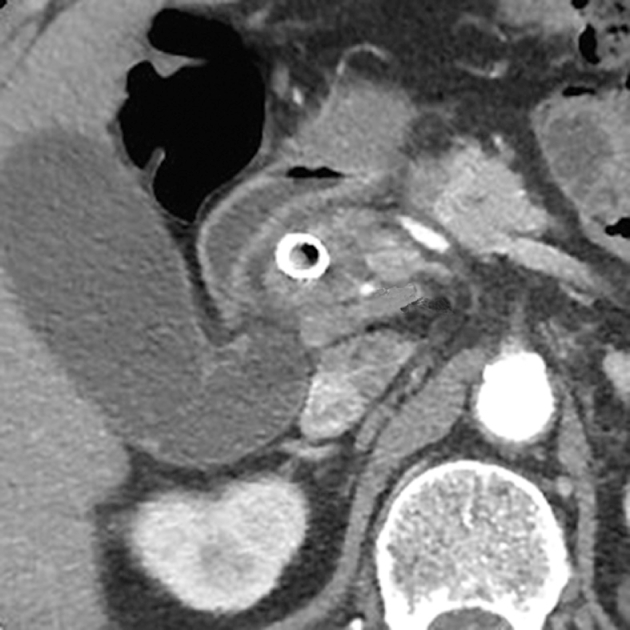
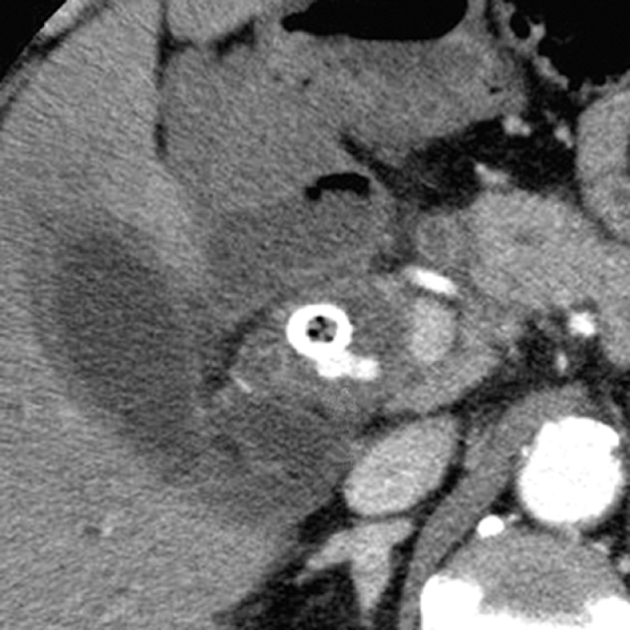
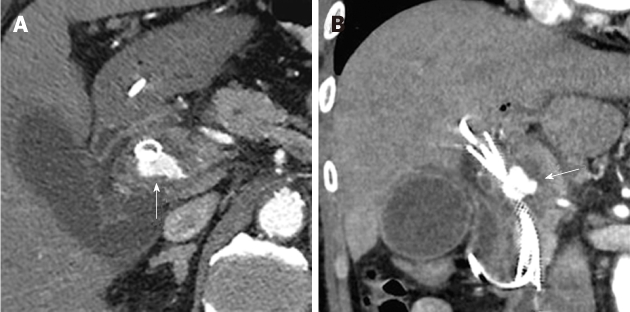
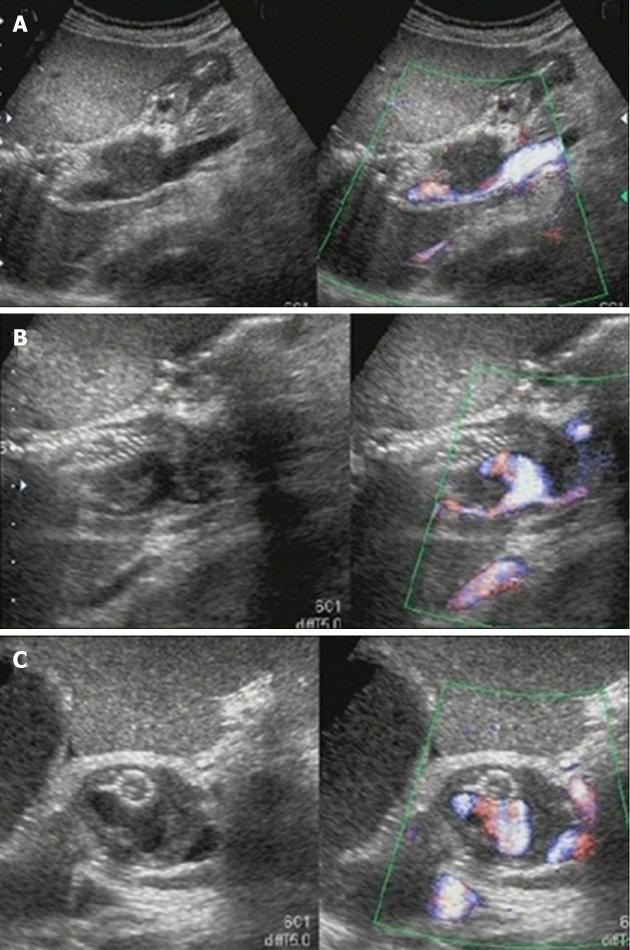
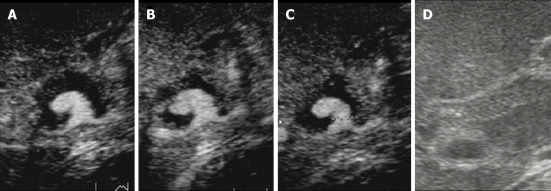
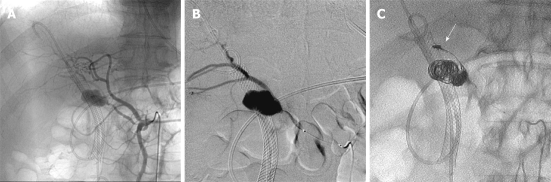
We report a case of a pseudoaneurysm of the right hepatic artery observed 9 mo after the endoscopic placement of a Wallstent, for bile duct stenosis, which was treated with transcatheter arterial embolization. The patient presented with obstructive jaundice and was diagnosed with inoperable common bile duct cancer. A plastic stent was inserted endoscopically to drain the bile, and chemotherapy was initiated. Abdominal pain and jaundice appeared approximately 6 mo after the beginning of chemotherapy. A diagnosis of stent occlusion and cholangitis was made, and the plastic stent was removed and substituted with a self-expandable metallic stent (SEMS) endoscopically. Nine months after SEMS insertion, contrast-enhanced computed tomography showed a pseudoaneurysm of the right hepatic artery protruding into the common bile duct lumen and in contact with the SEMS. The shape and size of the pseudoaneurysm and diameter of its neck was determined by contrast-enhanced ultrasonography using Sonazoid. A micro-catheter was led into the pseudoaneurysm in the right hepatic artery, GDC™ Detachable Coils were placed, and IDC™ Detachable Coils were then placed in the right hepatic artery on the distal and proximal sides of the pseudoaneurysm using the isolation method. There have been a few reports on pseudoaneurysm associated with stent placement in the biliary tract employing percutaneous transhepatic procedures, however, reports of pseudoaneurysms associated with endoscopic SEMS placement are very rare.
Keywords: Pseudoaneurysm; Self-expandable metallic stents; Sonazoid; Transcatheter arterial embolization; Wallstent.
Figures
References
-
- Rossi P, Bezzi M, Salvatori FM, Maccioni F, Porcaro ML. Recurrent benign biliary strictures: management with self-expanding metallic stents. Radiology. 1990;175:661–665. - PubMed
-
- Tesdal IK, Jaschke W, Duber C, Werhand J, Klose KJ. Biliary stenting: self-expandable and balloon-expandable stent. Early and late results. In: Liermann DD, editor. Stents-State of the art and future developments. Canada: Polyscience Publications Inc; 1995. pp. 190–195.
-
- Green MH, Duell RM, Johnson CD, Jamieson NV. Haemobilia. Br J Surg. 2001;88:773–786. - PubMed
-
- Sarr MG, Kaufman SL, Zuidema GD, Cameron JL. Management of hemobilia associated with transhepatic internal biliary drainage catheters. Surgery. 1984;95:603–607. - PubMed
-
- Hoevels J, Nilsson U. Intrahepatic vascular lesions following nonsurgical percutaneous transhepatic bile duct intubation. Gastrointest Radiol. 1980;5:127–135. - PubMed
LinkOut - more resources
Full Text Sources
