

doi: 10.1007/s12070-011-0159-0.
Epub 2011 Feb 23.
Endoscopic anatomy of the middle ear
Affiliations
- PMID: 22468244
- PMCID: PMC3102170
- DOI: 10.1007/s12070-011-0159-0
Item in Clipboard
Endoscopic anatomy of the middle ear
Indian J Otolaryngol Head Neck Surg.
2011 Apr.
Abstract
Good knowledge of anatomy is fundamental for every surgeon. Middle ear anatomy is really complex and sometimes is challenging for otologists, who need to explore every single compartment for a radical removal of pathology. With introduction of the endoscope in middle ear surgery, anatomy of middle ear spaces has become wider and clearer due to a better magnification and to the possibility to look "behind the corner". This article is a review of the state-of-art of endoscopic middle ear anatomy with description of every compartment, with particular attention to ventilation pathways and middle ear folds.
Keywords: Anatomy; Endoscope; Middle-ear.
Figures
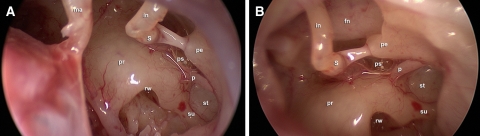
a–b Endoscopic anatomy of the sinus tympani during a transcanal approach. st Sinus tympani, p ponticulus, su subiculum, rw round window, pr promontory, ps posterior sinus, ma malleus, s stapes, in incus, pe pyramidal eminence, fn facial nerve
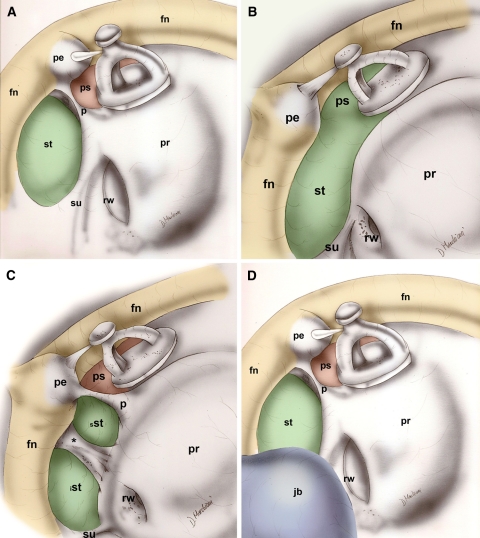
Different morphologic types of the ST. a classical shape, b confluent shape, c partitioned shape, d restricted shape. st Sinus tympani, p ponticulus, rw round window, pr promontory, ps posterior sinus, s stapes, su subiculum, pe pyramidal eminence, fn facial nerve, jb jugular bulb, *ridge of bone separating the sinus tympani
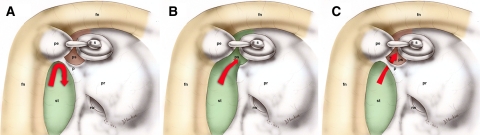
Different morphologies of ponticulus. a classical morphology, b incomplete ponticulus, c communicating ponticulus. st Sinus tympani, p ponticulus, rw round window, pr promontory, ps posterior sinus, s stapes, pe pyramidal eminence, fn facial nerve
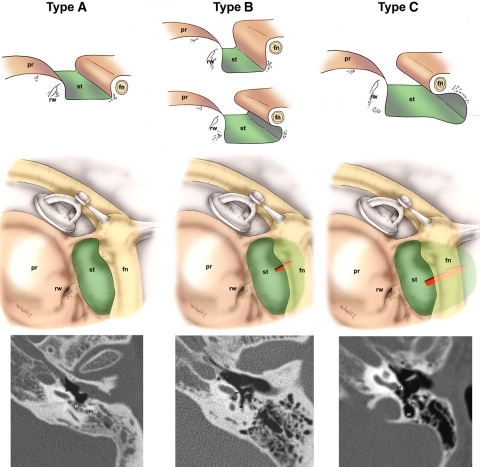
Classification ST’s depth based on axial CT scan. a limited sinus tympani, b deep sinus tympani with medially extension respect the facial nerve; c deep sinus tympani with posterior extension respect the facial nerve. fn Facial nerve, pr promontory, rw round window, st sinus tympani
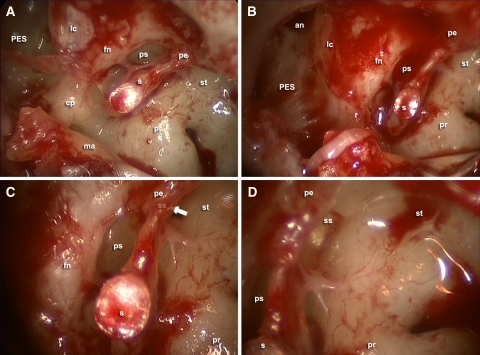
The subpyramidal space. a–b retrotympanic space with endoscope 45° angle view in a subject with a confluent shape of the ST; c magnification of posterior sinus and subpyramidal space (arrow); d exploration of subpyramidal space laying under the pyramidal eminence. st Sinus tympani, pr promontory, ps posterior sinus, s stapes, pe pyramidal eminence, fn facial nerve, lc lateral semicircular canal, an antrum, ss subpyramidal space, PES posterior epitympanic space, cp cochleariform process, ma malleus
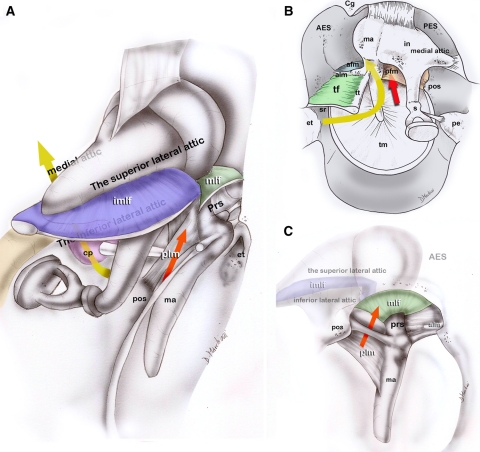
Epitympanic spaces and their ventilation routes. a posterior view; b medial to laterally view; c: lateral view. Long curved arrow ventilation route of the epitympanic-mastoid compartments, short arrow ventilation route of the Prussack space, ma Malleus, in incus, s stapes, cp cochleariform process, AES anterior epitympanic space, PES posterior epitympanic space, pos posterior spine, et Eustachian tube, imlf lateral incudomalleal fold, mlf lateral malleal fold, tf tensor fold, plm posterior malleal ligamental folds, alm anterior malleal ligamental folds
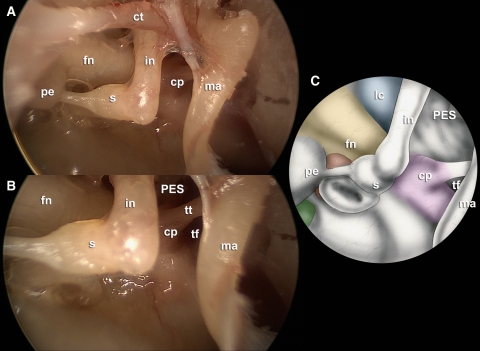
Tympanic isthmus. a magnification of the isthmus with a 0° endoscope; b magnification of the isthmus with a 45° angle endoscope; c scheme of the isthmus. ma Malleus, in incus, s stapes, cp cochleariform process, tt tensor tendon of the malleus, PES posterior epitympanic space, ct corda tympani, tf tensor fold, fn facial nerve, pe pyramidal eminence, lc lateral semicircular canal
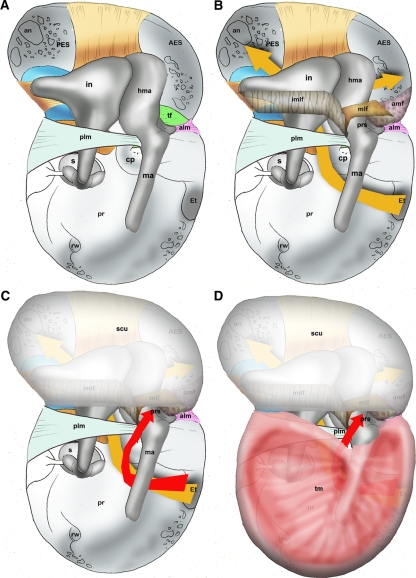
The two independent ventilation routes of the middle ear. a–b ventilation route to the epitympanic compartments through the isthmus (long arrow); c–d ventilation route to the Prussak’s space through the posterior pouch (short arrow). ma Malleus, hma head of the malleus, in incus, s stapes, cp cochleariform process, AES anterior epitympanic space, PES posterior epitympanic space, pos posterior spine, et Eustachian tube, imlf lateral incudomalleal fold, mlf lateral malleal fold, tf tensor fold, plm posterior malleal ligamental folds, alm anterior malleal ligamental folds, pr promontory, rw round window, scu scutum, prs prussack space, tm tympanic membrane, af anterior fold of the malleus
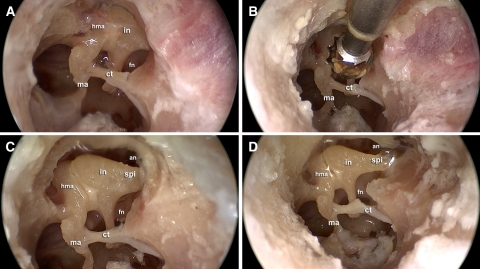
Endoscopic dissection view. Short process of the incus is a landmark for the antrum. a left ear after atticotomy with uncovered incudo-malleolar joint; b drilling the posterior portion of the scutum over the short process of the incus; c short process of the incus showing where the antrum is located; d relationship between the antrum and the short process of the incus after removing attic’s lateral bony wall. ma Malleus, hma head of the malleus, in incus, fn facial nerve, ct corda tympani, an antrum, spl short process of the incus
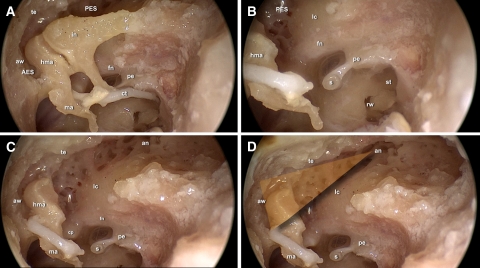
Endoscopic dissection demonstrating the epitympanic triangle. a left ear after removing attic’s lateral bony wall; b incus removal. Second tract of the facial nerve is a landmark for the lateral semicircular canal (it lies superiorly and posteriorly to the second tract of the facial nerve); c–d limits of the triangle defined superiorly by the tegmen tympani, anteriorly by the anterior bony wall of the AES and inferiorly by the lateral semicircular canal orientation. Tip of the triangle shows were the antrum is located. ma Malleus, hma head of the malleus, in incus, s stapes, fn facial nerve, ct corda tympani, an antrum, pe pyramidal eminence, PES posterior epitympanic space, AES anterior epitympanic space, lc lateral semicircular canal, te tegmen, aw anterior bony wall of AES
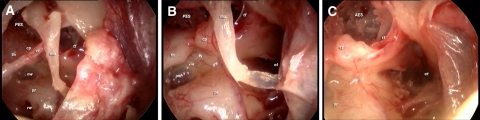
Endoscopic dissection showing the floor of epitympanic compartments (second tract of facial nerve, cochleariform process and tensor fold) after incus and stapes removal. a 45° endoscope view showing an incomplete tensor fold with a direct communication from the protympanic space to the anterior epitympanic space; b magnification of the tensor fold area with a 45° endoscope; c anatomy of the tensor fold after malleus removal. This picture shows the relationship between the protympanic space and the AES through the tensor fold. ma Malleus, s stapes, fn facial nerve, ct corda tympani, PES posterior epitympanic space, AES anterior epitympanic space, tf tensor fold, pr promontory, et Eustachian tube, cp cochlear process, rw round window, ow oval window
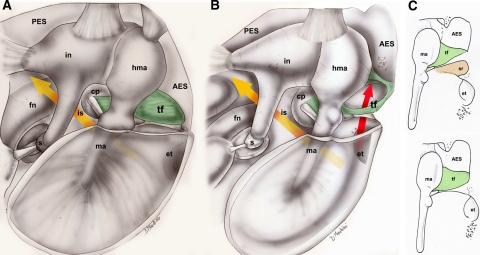
Anatomy and variations of the tensor fold. a subject with a complete tensor fold separating AES from protympanum, the only aeration pathway to the epitympanum is through the isthmus (long arrow); b subject with an incomplete tensor fold, an additional ventilation route through the tensor fold is present in this case (short arrow); c1 Onal AES type I consisting of two cavities separated by the tensor tympani fold, the supratubal recess inferiorly and the anterior malleal space superiorly. c2 Onal AES type II consisting of one single cavity anterior to the head of the malleus, in this case the supratubal recess is not present. ma Malleus, hma head of the malleus, in incus, s stapes, fn facial nerve, PES posterior epitympanic space, AES anterior epitympanic space, tf tensor fold, et Eustachian tube, cp cochlear process, is isthmus, sr supratubal recess
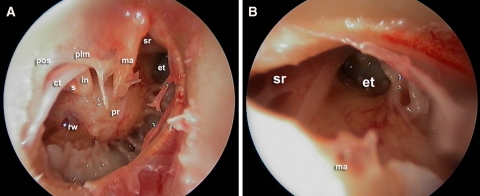
Supratubal recess view with a 45° endoscope in the protympanic space. a right ear with wide perforation of the drum; b magnification of the protympanum with a good view of the anatomic relationship between Eustachian tube and the supratubal recess. ma Malleus, in incus, s stapes, et Eustachian tube, sr supratubal recess, ct corda tympani, pos posterior spine, rw round window, pr promontory, plm posterior malleal ligamental folds
References
-
- Reuter HJ. Philipp Bozzini and endoscopy in the 19th Century. Stuttgart: Max Nitze Museum; 1988.
LinkOut - more resources
Full Text Sources