

doi: 10.3201/eid1804.111478.
Identification of risk factors for chronic Q fever, the Netherlands
Affiliations
- PMID: 22469535
- PMCID: PMC3309671
- DOI: 10.3201/eid1804.111478
Item in Clipboard
Identification of risk factors for chronic Q fever, the Netherlands
Emerg Infect Dis.
2012 Apr.
Abstract
Since 2007, the Netherlands has experienced a large Q fever outbreak. To identify and quantify risk factors for development of chronic Q fever after Coxiella burnetii infection, we performed a case-control study. Comorbidity, cardiovascular risk factors, medications, and demographic characteristics from 105 patients with proven (n = 44), probable (n = 28), or possible (n = 33) chronic Q fever were compared with 201 patients who had acute Q fever in 2009 but in whom chronic Q fever did not develop (controls). Independent risk factors for development of proven chronic Q fever were valvular surgery, vascular prosthesis, aneurysm, renal insufficiency, and older age.
Figures
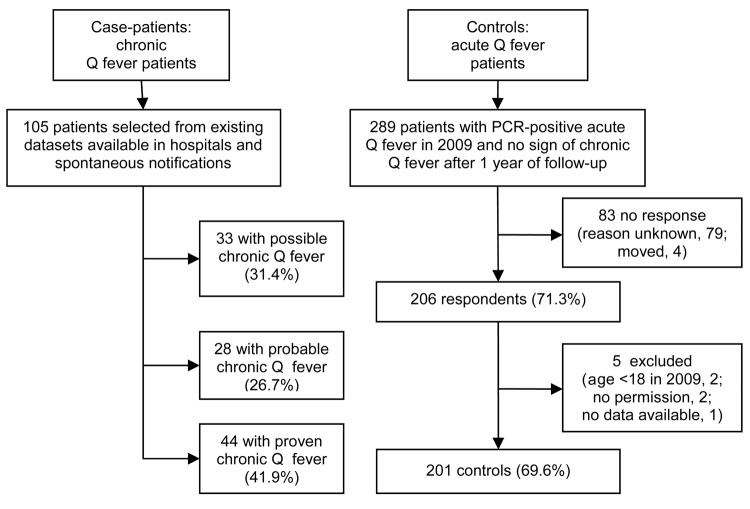
Enrollment, selection, and inclusion criteria forcase-patients and controls for case–control study to identify risk factors for chronic Q fever, the Netherlands.
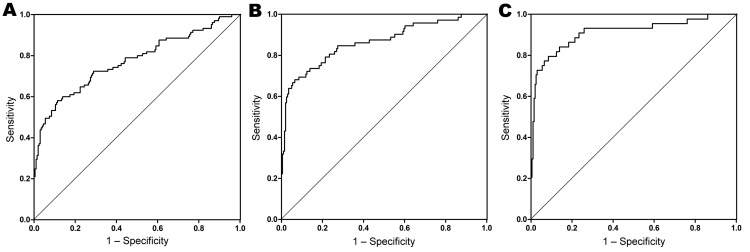
Goodness-of-fit models for case–control study to identify risk factors for chronic Q fever, the Netherlands. A) All chronic Q fever cases (n = 105); area under the curve (c-statistic) 0.77 (95% CI 0.71–0.83); p<0.001. B) Proven and probable chronic Q fever cases (n = 72); c-statistic 0.86 (95% CI 0.81–0.92); p<0.001. C) Proven chronic Q fever cases (n = 44); c-statistic 0.91 (95% CI 0.85–0.97); p<0.001. Patient risk factors included in the model (no. observations): A) valvular surgery (18); vascular prosthesis (15); aneurysm (12); nonhematologic malignancy (16); age, continuous, mean 63.9 y; B) valvular surgery (18); vascular prosthesis (15); aneurysm (12); renal insufficiency (12); age, continuous, mean 67.3 y; C) valvular surgery (10); vascular prosthesis (14); aneurysm (9); renal insufficiency (9); age, continuous, mean 68.4.
References
MeSH terms
LinkOut - more resources
Full Text Sources