

Transsphenoidal resection of sellar tumors using high-field intraoperative magnetic resonance imaging
- PMID: 22470265
- PMCID: PMC3312115
- DOI: 10.1055/s-0031-1277262
Transsphenoidal resection of sellar tumors using high-field intraoperative magnetic resonance imaging
Abstract
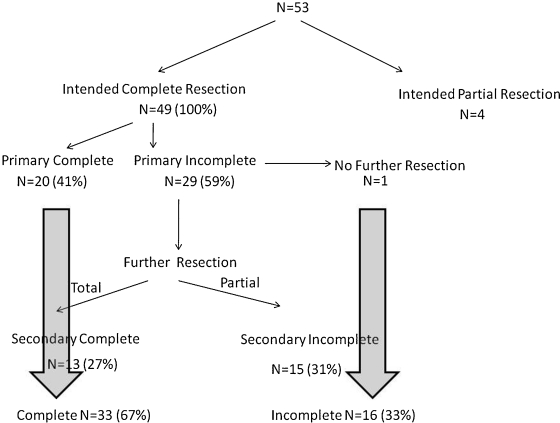
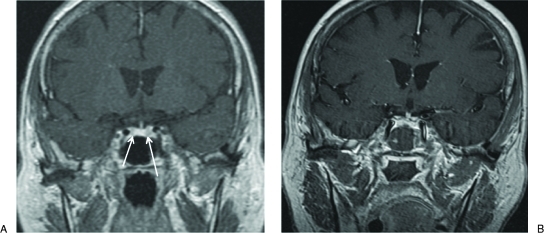
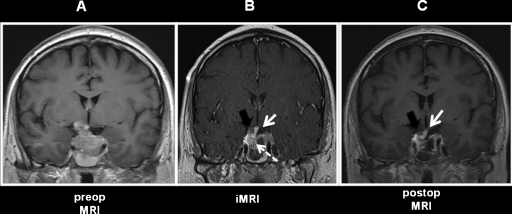
There has been increasing experience in the utilization of intraoperative magnetic resonance imaging (iMRI) for intracranial surgery. Despite this trend, only a few U.S centers have examined the use of this technology for transsphenoidal resection of tumors of the sella. We present the largest series in North America examining the role of iMRI for pituitary adenoma resection. We retrospectively reviewed our institutional experience of 59-patients who underwent transsphenoidal procedures for sellar and suprasellar tumors with iMRI guidance. Of these, 52 patients had a histological diagnosis of pituitary adenoma. The technical results of this subgroup were examined. A 1.5-T iMRI was integrated with the BrainLAB (Feldkirchen, Germany) neuronavigation system. The majority (94%) of tumors in our series were macroadenomas. Seventeen percent of tumors were confined to the sella, 49% had suprasellar extensions without involvement of the cavernous sinus, 34% had frank cavernous sinus invasion. All patients underwent at least one iMRI, and 19% required one or more additional sets of intraoperative imaging. In 58% of patients, iMRI led to the surgeon attempting more resection. A gross total resection was obtained in 67% of the patients with planned total resections. There was one case of permanent postoperative diabetes insipidus and no other instances of new hormone replacement. In summary, iMRI was most useful for tumors of the sella with and without suprasellar extension where the information from the iMRI extended the complete resection rate from 40 to 72% and 55 to 88%, respectively. As one would expect, it did not substantially increase the rate of resection of tumors with cavernous sinus invasion. Overall, iMRI was particularly useful in guiding resection safely, aiding in clinical decision making, and allowing identification and preservation of the pituitary stalk and normal pituitary gland. Limitations of the iMRI include a need for additional personnel and training as well as additional operative time, which diminishes over time as personnel learn to optimize workflow efficiency. Additional costs are mitigated in part by using the iMRI as an immediate postoperative scan. Other data emerging from our experience suggest that preservation of normal gland and thus avoidance of hypopituitarism may be improved by iMRI use, but longer follow-up periods are required to test this conclusion. iMRI can detect unsuspected complications sooner than routine postoperative imaging, potentially leading to improved outcomes. However, larger studies are needed.
Keywords: Intraoperative MRI; pituitary; transsphenoidal.
Figures
Similar articles
-
Transsphenoidal pituitary macroadenomas resection guided by PoleStar N20 low-field intraoperative magnetic resonance imaging: comparison with early postoperative high-field magnetic resonance imaging.Neurosurgery. 2009 Jul;65(1):63-70; discussion 70-1. doi: 10.1227/01.NEU.0000348549.26832.51. Neurosurgery. 2009. PMID: 19574826
-
Intraoperative high-field MRI for transsphenoidal reoperations of nonfunctioning pituitary adenoma.J Neurosurg. 2014 Nov;121(5):1166-75. doi: 10.3171/2014.6.JNS131994. Epub 2014 Aug 15. J Neurosurg. 2014. PMID: 25127413
-
Characterization of tumor remnants in intraoperative MRI-assisted microscopic and endoscopic transsphenoidal resection of less invasive pituitary adenomas.Neurosurg Rev. 2022 Apr;45(2):1701-1708. doi: 10.1007/s10143-021-01705-z. Epub 2021 Dec 2. Neurosurg Rev. 2022. PMID: 34855027 Free PMC article.
-
Intraoperative magnetic resonance imaging assessment of non-functioning pituitary adenomas during transsphenoidal surgery.Pituitary. 2016 Apr;19(2):222-31. doi: 10.1007/s11102-015-0679-9. Pituitary. 2016. PMID: 26323592 Review.
-
Intra-operative MRI vs endoscopy in achieving gross total resection of pituitary adenomas: a systematic review.Acta Neurochir (Wien). 2019 Aug;161(8):1683-1698. doi: 10.1007/s00701-019-03955-9. Epub 2019 May 28. Acta Neurochir (Wien). 2019. PMID: 31139934
Cited by
-
Development and prospective validation of an artificial intelligence-based smartphone app for rapid intraoperative pituitary adenoma identification.Commun Med (Lond). 2024 Mar 13;4(1):45. doi: 10.1038/s43856-024-00469-z. Commun Med (Lond). 2024. PMID: 38480833 Free PMC article.
-
The utility of high-resolution intraoperative MRI in endoscopic transsphenoidal surgery for pituitary macroadenomas: early experience in the Advanced Multimodality Image Guided Operating suite.Neurosurg Focus. 2016 Mar;40(3):E18. doi: 10.3171/2016.1.FOCUS15515. Neurosurg Focus. 2016. PMID: 26926058 Free PMC article.
-
Do We Need Intraoperative Magnetic Resonance Imaging in All Endoscopic Endonasal Pituitary Adenoma Surgery Cases? A Retrospective Study.Front Oncol. 2021 Oct 1;11:733838. doi: 10.3389/fonc.2021.733838. eCollection 2021. Front Oncol. 2021. PMID: 34660296 Free PMC article.
-
iMRI During Transsphenoidal Surgery.Neurosurg Clin N Am. 2017 Oct;28(4):499-512. doi: 10.1016/j.nec.2017.05.005. Epub 2017 Aug 18. Neurosurg Clin N Am. 2017. PMID: 28917279 Free PMC article. Review.
-
Consensus guideline for the diagnosis and management of pituitary adenomas in childhood and adolescence: Part 1, general recommendations.Nat Rev Endocrinol. 2024 May;20(5):278-289. doi: 10.1038/s41574-023-00948-8. Epub 2024 Feb 9. Nat Rev Endocrinol. 2024. PMID: 38336897 Review.
References
-
- Yeh P J, Chen J W. Pituitary tumors: surgical and medical management. Surg Oncol. 1997;6:67–92. - PubMed
-
- Kaltsas G A, Evanson J, Chrisoulidou A, Grossman A B. The diagnosis and management of parasellar tumours of the pituitary. Endocr Relat Cancer. 2008;15:885–903. - PubMed
-
- De Tommasi C, Vance M L, Okonkwo D O, Diallo A, Laws E R., Jr Surgical management of adrenocorticotropic hormone-secreting macroadenomas: outcome and challenges in patients with Cushing's disease or Nelson's syndrome. J Neurosurg. 2005;103:825–830. - PubMed
-
- Jagannathan J, Sheehan J P, Pouratian N, Laws E R, Jr, Steiner L, Vance M L. Gamma knife radiosurgery for acromegaly: outcomes after failed transsphenoidal surgery. Neurosurgery. 2008;62:1262–1269. discussion 1269–1270. - PubMed
-
- Cohen-Gadol A A, Liu J K, Laws E R., Jr Cushing's first case of transsphenoidal surgery: the launch of the pituitary surgery era. J Neurosurg. 2005;103:570–574. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
