

Increased sleep fragmentation leads to impaired off-line consolidation of motor memories in humans
- PMID: 22470524
- PMCID: PMC3314699
- DOI: 10.1371/journal.pone.0034106
Increased sleep fragmentation leads to impaired off-line consolidation of motor memories in humans
Abstract
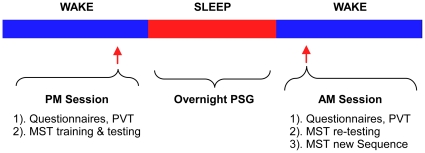
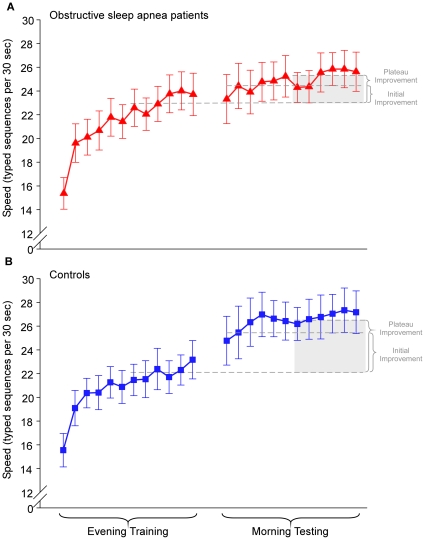
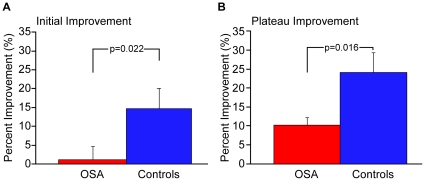
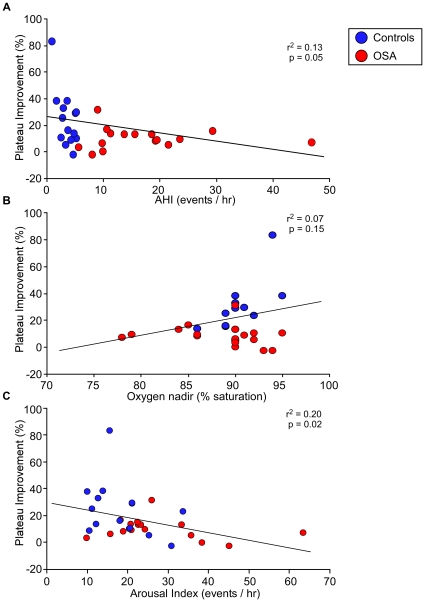
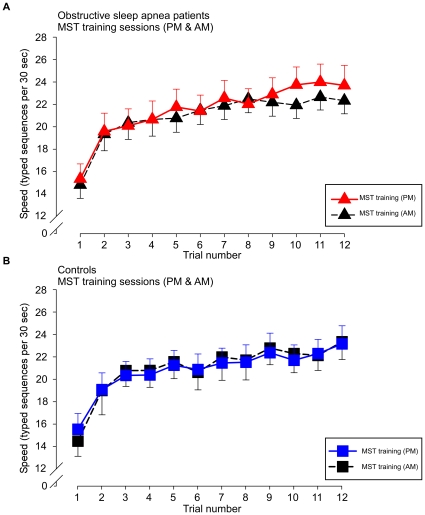
A growing literature supports a role for sleep after training in long-term memory consolidation and enhancement. Consequently, interrupted sleep should result in cognitive deficits. Recent evidence from an animal study indeed showed that optimal memory consolidation during sleep requires a certain amount of uninterrupted sleep. Sleep continuity is disrupted in various medical disorders. We compared performance on a motor sequence learning task (MST) in relatively young subjects with obstructive sleep apnea (n = 16; apnea-hypopnea index 17.1±2.6/h [SEM]) to a carefully matched control group (n = 15, apnea-hypopnea index 3.7±0.4/h, p<0.001. Apart from AHI, oxygen nadir and arousal index, there were no significant differences between groups in total sleep time, sleep efficiency and sleep architecture as well as subjective measures of sleepiness based on standard questionnaires. In addition performance on the psychomotor vigilance task (reaction time and lapses), which is highly sensitive to sleep deprivation showed no differences as well as initial learning performance during the training phase. However there was a significant difference in the primary outcome of immediate overnight improvement on the MST between the two groups (controls = 14.7±4%, patients = 1.1±3.6%; P = 0.023) as well as plateau performance (controls = 24.0±5.3%, patients = 10.1±2.0%; P = 0.017) and this difference was predicted by the arousal index (p = 0.02) rather than oxygen saturation (nadir and time below 90% saturation. Taken together, this outcome provides evidence that there is a clear minimum requirement of sleep continuity in humans to ensure optimal sleep dependent memory processes. It also provides important new information about the cognitive impact of obstructive sleep apnea and challenges its current definitions.
Conflict of interest statement
Figures
References
-
- Stickgold R, James L, Hobson JA. Visual discrimination learning requires sleep after training. Nat Neurosci. 2000;3:1237–1238. - PubMed
-
- Maquet P, Laureys S, Peigneux P, Fuchs S, Petiau C, et al. Experience-dependent changes in cerebral activation during human REM sleep. Nat Neurosci. 2000;3:831–836. - PubMed
-
- Diekelmann S, Born J. The memory function of sleep. Nat Rev Neurosci. 2010;11:114–126. - PubMed
-
- Stickgold R. Sleep-dependent memory consolidation. Nature. 2005;437:1272–1278. - PubMed
-
- Willingham DB. A neuropsychological theory of motor skill learning. Psychol Rev. 1998;105:558–584. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
