

doi: 10.3941/jrcr.v4i10.512.
Epub 2010 Oct 1.
Sinistral portal hypertension: presentation, radiological findings, and treatment options - a case report
Affiliations
- PMID: 22470692
- PMCID: PMC3303351
- DOI: 10.3941/jrcr.v4i10.512
Item in Clipboard
Sinistral portal hypertension: presentation, radiological findings, and treatment options - a case report
J Radiol Case Rep.
2010.
Abstract
Sinistral portal hypertension occurs when a pathological process causes occlusion of the splenic vein. The resultant elevated splenic bed venous pressure causes formation of gastric varices which can lead to hematemesis as a common presentation for this disease process. We present a case of sinistral portal hypertension in a patient with acute hematemesis as the primary presentation. Despite the challenging diagnosis process, the patient underwent splenectomy and was managed appropriately according to previously published literature.
Keywords: Sinistral hypertension; UGI bleed; left-sided portal hypertension; pancreatitis; upper gastro intestinal bleeding.
Figures

34 year old male with acute onset of hematemesis due to sinistral portal hypertension. Relevant CT scan findings in Portal Venous Phase: Varices (arrow) (a). Soft tissue thickening in splenic hilum (arrow) (b). Splenic vein incomplete filling (arrow) (c, d) on coronal view. Areas of suspected pathology magnified in insert of each corresponding image. (Protocol: Siemens Sensation 64, 3mm slice thickness, 120 kVp 369 mA, Omnipaque 350, 120 cc)
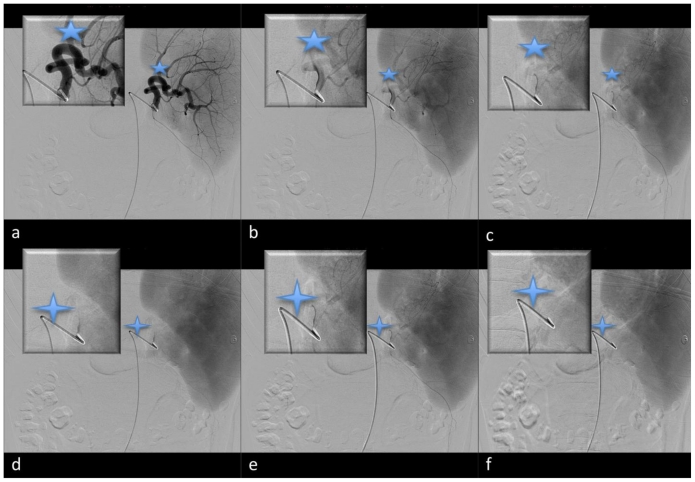
34 year old male with acute onset of hematemesis due to sinistral portal hypertension. Splenic angiography. Arterial phase (a,c) (five point star) illustrates patent splenic artery. There is an absence of splenic vein filling following splenic artery injection with contrast as depicted by (d-f) (four point star). Corresponding magnified image of the hilum provided in each image insert. (Protocol: Flouroscopy, Philips, Visipaque, 130cc, fluoro time 34.6 minutes, access made through Right femoral artery, selective splenic artery catheterization with a 4Fr Glide Catheter (Terumo, Japan), rate of injection 5 cc/sec, total volume 30 cc, contrast injection made in distal splenic artery proximal to splenic hilum)

34 year old male with acute onset of hematemesis due to sinistral portal hypertension. Soft tissue stranding of splenic hilum suggestive of possible silent chronic pancreatitis (arrow) (a). Splenic vein filling defect (Portal Venous phase shown), initially inconclusive, supported distal splenic vein thrombosis following splenic angiogram illustrated above (arrow) (b,c,d). Areas of suspected pathology magnified in insert of each corresponding image. (Protocol: Siemens Sensation 64, 3mm slice thickness, 120 kVp, 369 mA, Omnipaque 350, 120 cc)
References
-
- Singhal D, Kakodkar R, Soin A, Gupta S, Nundy S. Sinistral Portal Hypertension. A Case Report. JOP. 2006;7(6):670–67. - PubMed
-
- Koklu S, Coban S, Yuksel O, Arhan M. Left-Sided Portal Hypertension. Dig Dis Sci. 2007;52:1141–1149. - PubMed
-
- Cakamak O, Parildar M, Oran I, Sever A, Memis A. Sinistral Portal Hypertension; imaging findings and endovascular therapy. Abdom Imaging. 2006;30:208–213. - PubMed
-
- Agarwal A, Kumar R, Agarwal S, Sing S. Significane of Splenic Vein Thrombosis in Chroinc Pancreatitis. Am J Surg. 2008;196:149–154. - PubMed
LinkOut - more resources
Full Text Sources