

doi: 10.3941/jrcr.v4i8.476.
Epub 2010 Aug 1.
Coexisting MS and Lhermitte-Duclos Disease
Affiliations
- PMID: 22470746
- PMCID: PMC3303393
- DOI: 10.3941/jrcr.v4i8.476
Item in Clipboard
Coexisting MS and Lhermitte-Duclos Disease
J Radiol Case Rep.
2010.
Abstract
We report the case of a patient with pre-existing multiple sclerosis, who presented with horizontal diplopia, and a prior episode of progressive ataxia and dizziness lasting one week. While initially attributed to multiple sclerosis, subsequent imaging demonstrated a concurrent left cerebellar gangliocytoma, also known as Lhermitte-Duclos disease.
Keywords: Lhermitte-Duclos disease; Multiple Sclerosis; cerebellar gangliocytoma.
Figures

41 yo female with history of multiple sclerosis presented with horizontal diplopia. Noncontrast enhanced axial CT slices (64 slice Somatom, Siemens Health Care, Erlangen, Germany, 3 mm axial reconstruction, 440 mA, 120 KVp) demonstrate a predominantly hypodense lesion in the left cerebellar hemisphere sparing the cerebellar peduncle with slight mass effect upon the fourth ventricle.
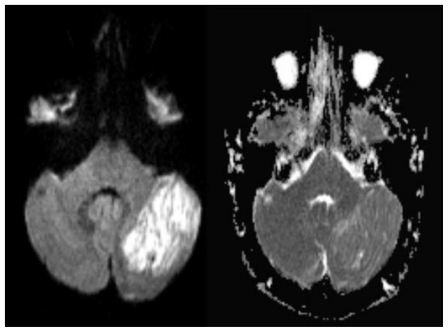
41 yo female with history of multiple sclerosis presented with horizontal diplopia. Axial diffusion weighted imaging (left image, B-1000)(1.5 Tesla Siemens Espree, repetition time (TR) = 4500 ms; echo time (TE) = 112 ms) demonstrates a 3 × 4 cm large, well defined area of predominantly corduroy appearing, increased signal in the left cerebellar hemisphere with sparing of the cerebellar peduncle, causing slight mass effect upon the left aspect of the 4th ventricle. Corresponding apparent diffusion coefficient (ADC) map (right image) shows increased diffusion values proving lack of diffusion restriction. This excludes acute ischemia and is typically found in LDD. Medulloblastoma that may present with diffusion restriction becomes a less likely differential diagnosis.
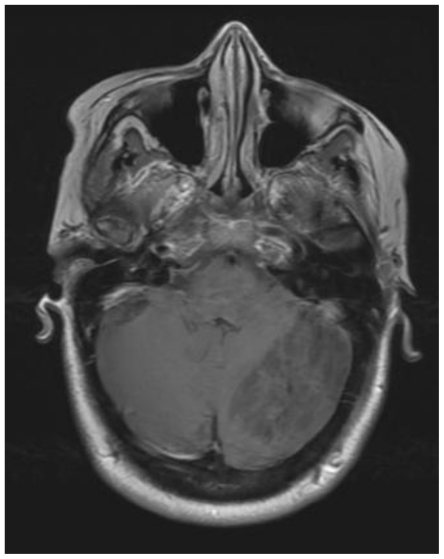
41 yo female with history of multiple sclerosis presented with horizontal diplopia. This axial T1-weighted image (General Electric Signa 3.0Tesla; TR = 2607ms, TE = 9.94 ms, inversion time (TI) 1100ms, number of excitations (NEX), 2; flip angle FA = 90) demonstrates alternating isointense and hypointense signal of the tumor within the left lobe of the cerebellum. This is the characteristic striated corduroy pattern of a tumor in Lhermitte-Duclos disease.
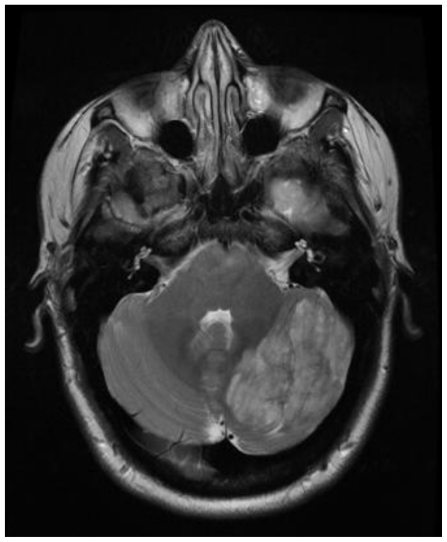
41 yo female with history of multiple sclerosis presented with horizontal diplopia. This axial T2-weighted image (General Electric Signa 3.0Tesla; TR = 5200ms, TE = 101.82 ms, number of excitations (NEX), 2; flip angle FA = 90) demonstrates alternating isointense and hyperintense signals of the tumor within the left lobe of the cerebellum. This is the characteristic striated pattern of a tumor in Lhermitte-Duclos disease. The adjacent cerebellar fissures are affected from associated mass effect.
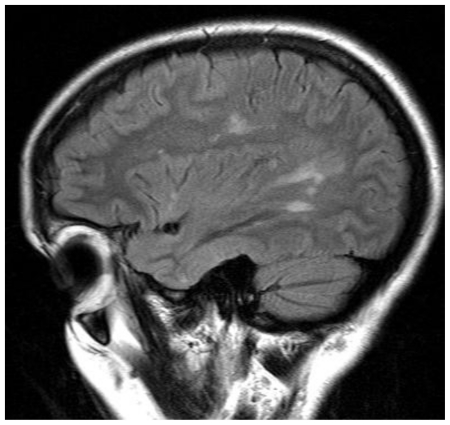
41 yo female with history of multiple sclerosis presented with horizontal diplopia. This sagittal FLAIR image (1.5 Tesla Siemens Espree, TR = 9000 ms; TE = 123 ms; inversion time TI = 2500 ms; FA 180) demonstrates hyperintense lesions along the corona radiata and extending into the corpus callosum suggestive of Dawson’s fingers, which are characteristic of MS plaques. Subsequent images (see Figure 6) demonstrated Lhermitte-Duclos disease in concurrence with MS.
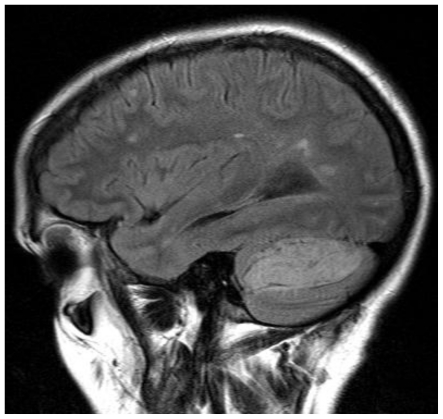
41 yo female with history of multiple sclerosis presented with horizontal diplopia. This sagittal FLAIR (1.5 Tesla Siemens Espree, TR = 9000 ms; TE = 123 ms; TI = 2500 ms; FA 180) image demonstrates concurrent MS plaques along with a striated-appearing cerebellar tumor characteristic of Lhermitte-Duclos disease.
References
-
- Consortium of MS Centers MRI Protocol for the Diagnosis and Follow-up of MS. www.mscare.org.
-
- Grossman RI, Yousem DM. Neuroradiology: The Requisites. 2nd ed. Philadelphia: Mosby; 2003. pp. 137–138.pp. 143
-
- Robinson S, Cohen A. Cowden Disease and Lhermitte-Duclos Disease, Neurosurgery. 2000;46(2):371–83. - PubMed
-
- Osborn AG. Brain. 1st ed. Section I-6. Salt Lake City: Amirsys; 2004. Diagnostic Imaging; pp. 70–3.
LinkOut - more resources
Full Text Sources