

Extramedullary duodenal plasmacytoma presenting with gastric outlet obstruction and painless jaundice
- PMID: 22470749
- PMCID: PMC3303390
- DOI: 10.3941/jrcr.v4i8.487
Extramedullary duodenal plasmacytoma presenting with gastric outlet obstruction and painless jaundice
Abstract
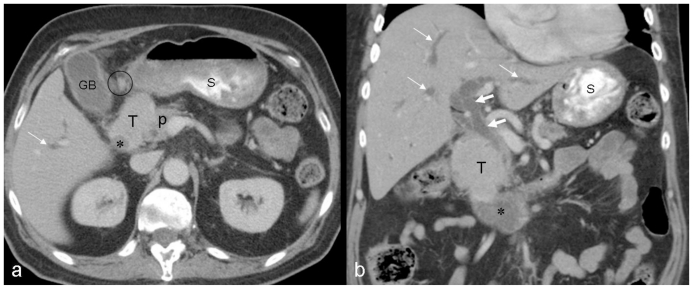
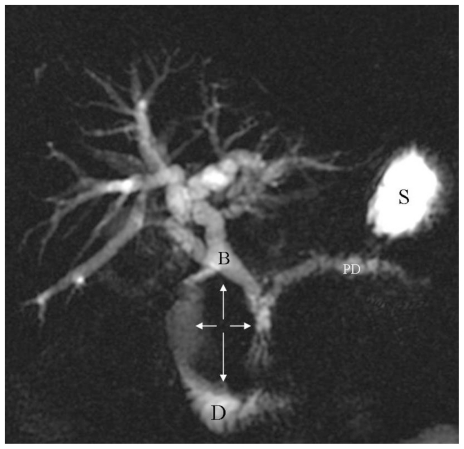
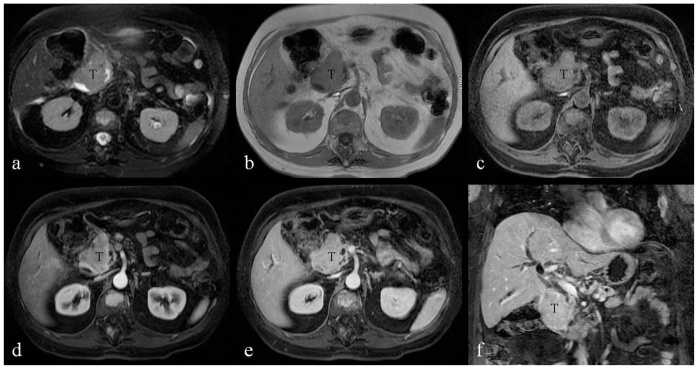
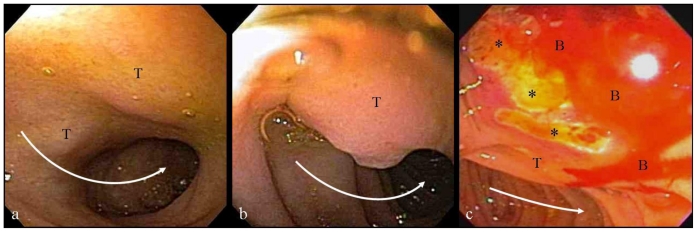
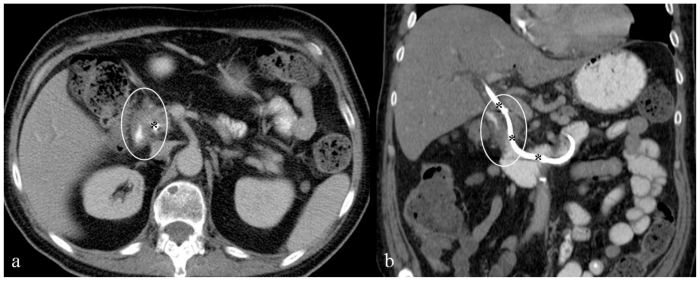
Malignant plasma cells in multiple myeloma are predominantly confined to the medullary space of the skeletal system, therefore the disease course will be dominated by signs and symptoms related to bone marrow infiltration and destructive bone lesions with their consequences as well as abnormal protein production. Visceral extramedullary plasmacytoma involving the gastrointestinal system and particularly the duodenum is a rare manifestation of the disease. We report a case of duodenal extramedullary plasmacytoma presenting with gastric outlet obstruction and painless jaundice, in a patient treated for multiple myeloma. Diagnosis was first suggested on imaging, and proved by endoscopic biopsy. The duodenal mass resolved following chemotherapy.
Keywords: Multiple myeloma; duodenal plasmacytoma; extramedullary multiple myeloma; gastric outlet obstruction; gastrointestinal involvement; painless jaundice.
Figures
References
-
- Pimmental R, vanstolk R. Gastric plasmacytoma: A rare cause of massive gastrointestinal bleeding. Am J Gastroenterol. 1993;88:1963–1964. - PubMed
-
- Chim CS, Wong WM, Nicholls J, Chung LP, Liang R. Extramedullary sites of invovelment in hematologic malignancies: case3. Hemorrhagic gastric plasmacytoma as the primary presentation in multiple myeloma. J Clin Oncol. 2002;20:344–347. - PubMed
-
- Alexiou C, Kau RJ, Dietzfelbinger H, et al. Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts. Cancer. 1999;85:2305–2314. - PubMed
-
- Goldstein WB, Poker N. Multiple myeloma involving the gastrointestinal tract. Gastroenterology. 1966;51:87–93. - PubMed
LinkOut - more resources
Full Text Sources