

Plunging ranula
- PMID: 22470797
- PMCID: PMC3303342
- DOI: 10.3941/jrcr.v5i6.682
Plunging ranula
Abstract
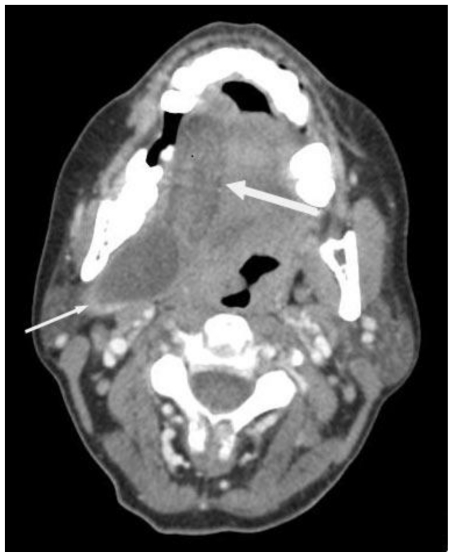
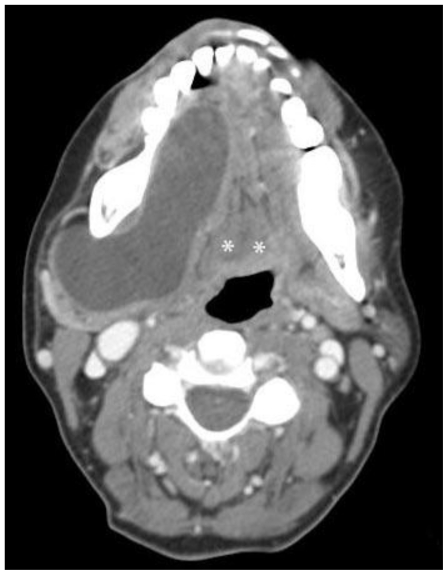
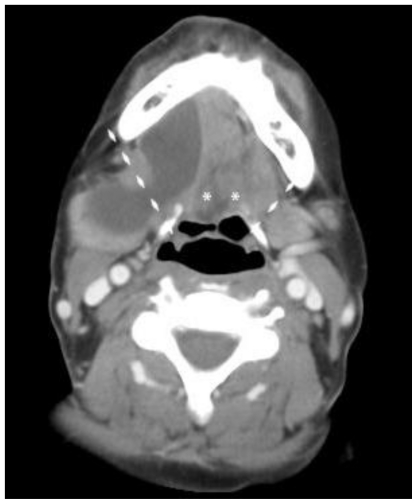
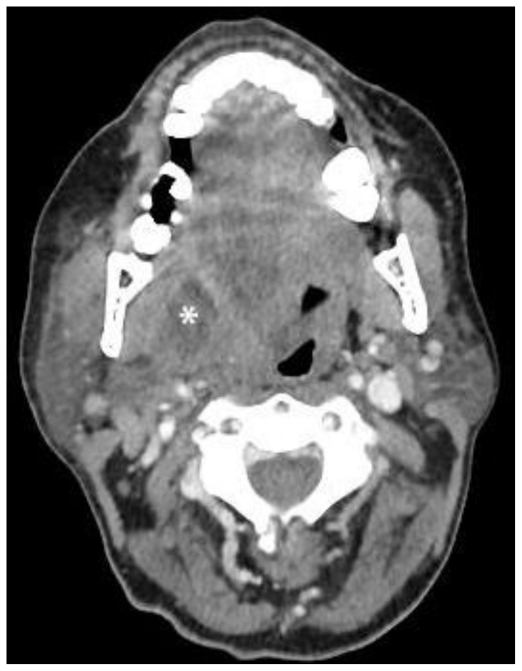
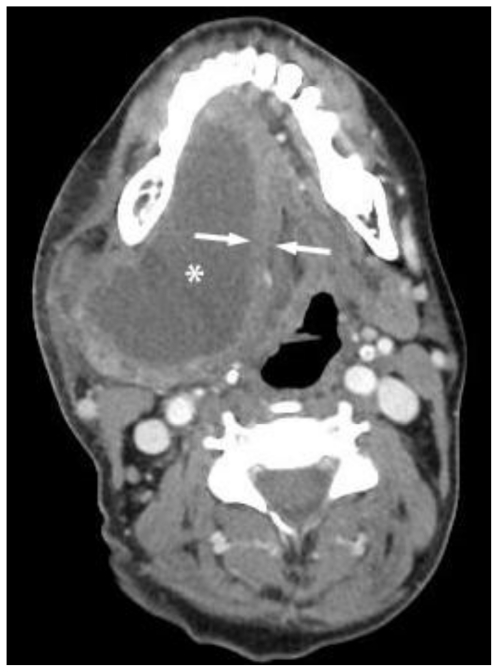
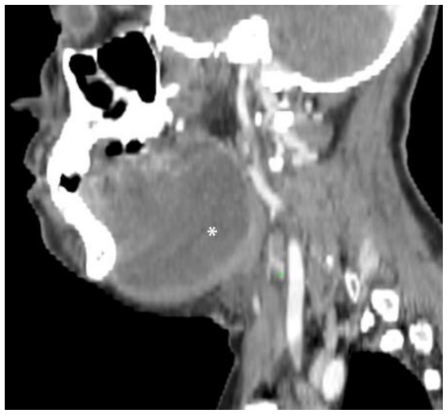
Plunging ranulas are rare cystic masses in the neck that are mucous retention pseudocysts from an obstructed sublingual gland. They "plunge" by extending inferiorly beyond the free edge of the mylohyoid muscle, or through a dehiscence of the muscle itself, to enter the submandibular space. Imaging demonstrates a simple cystic lesion in the characteristic location and can be used to delineate relevant surgical anatomy. Surgical excision of the collection and the involved sublingual gland is performed for definitive treatment. We present a case of plunging ranula in a 44 year old female who presented with a painless, slowly enlarged neck mass. Plunging ranulas should be considered in the differential diagnosis of cystic neck masses, specifically when seen extending over, or through, the mylohyoid muscle.
Keywords: cystic neck masses; diving ranula; plunging ranula; ranula.
Figures


References
-
- Coit WE, Harnsberger HR, Osborn AG, Smoker WR, Stevens MH, Lufkin RB. Ranulas and their mimics: CT evaluation. Radiology. 1987 Apr;163(1):211–6. - PubMed
-
- Davison MJ, Morton RP, McIvor NP. Plunging Ranula: clinical observations. Head Neck. 1998 Jan;20(1):63–8. - PubMed
-
- Morton RP, Ahmad Z, Jain P. Plunging ranula: congenital or acquired. Otolaryngol Head Neck Surg. 2010 Jan;142(1):104–7. - PubMed
-
- Charnoff SK, Carter BL. Plunging Ranula: CT diagnosis. Radiology. 1986 Feb;158(2):467–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources