

Errors in medication history at hospital admission: prevalence and predicting factors
- PMID: 22471836
- PMCID: PMC3353244
- DOI: 10.1186/1472-6904-12-9
Errors in medication history at hospital admission: prevalence and predicting factors
Abstract
Background: An accurate medication list at hospital admission is essential for the evaluation and further treatment of patients. The objective of this study was to describe the frequency, type and predictors of errors in medication history, and to evaluate the extent to which standard care corrects these errors.
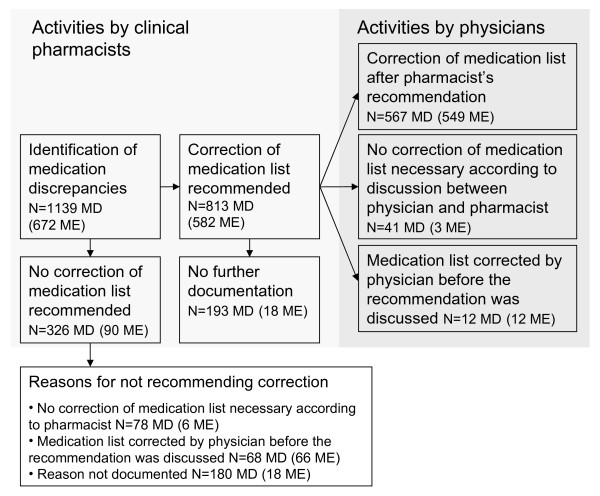
Methods: A descriptive study was carried out in two medical wards in a Swedish hospital using Lund Integrated Medicines Management (LIMM)-based medication reconciliation. A clinical pharmacist identified each patient's most accurate pre-admission medication list by conducting a medication reconciliation process shortly after admission. This list was then compared with the patient's medication list in the hospital medical records. Addition or withdrawal of a drug or changes to the dose or dosage form in the hospital medication list were considered medication discrepancies. Medication discrepancies for which no clinical reason could be identified (unintentional changes) were considered medication history errors.
Results: The final study population comprised 670 of 818 eligible patients. At least one medication history error was identified by pharmacists conducting medication reconciliations for 313 of these patients (47%; 95% CI 43-51%). The most common medication error was an omitted drug, followed by a wrong dose. Multivariate logistic regression analysis showed that a higher number of drugs at admission (odds ratio [OR] per 1 drug increase = 1.10; 95% CI 1.06-1.14; p < 0.0001) and the patient living in their own home without any care services (OR = 1.58; 95% CI 1.02-2.45; p = 0.042) were predictors for medication history errors at admission. The results further indicated that standard care by non-pharmacist ward staff had partly corrected the errors in affected patients by four days after admission, but a considerable proportion of the errors made in the initial medication history at admission remained undetected by standard care (OR for medication errors detected by pharmacists' medication reconciliation carried out on days 4-11 compared to days 0-1 = 0.52; 95% CI 0.30-0.91; p=0.021).
Conclusions: Clinical pharmacists conducting LIMM-based medication reconciliations have a high potential for correcting errors in medication history for all patients. In an older Swedish population, those prescribed many drugs seem to benefit most from admission medication reconciliation.
Figures
References
-
- Campbell F, Karnon J, Czoski-Murray C, Jones R. A systematic review of the effectiveness and cost-effectiveness of interventions aimed at preventing medication error (medicines reconciliation) at hospital admission. The University of Sheffield, School of Health and Related Research: Sheffield. 2007.
-
- World Health Organization. Assuring medication accuracy at transitions in care. Standard operating protocol fact sheet. Retrieved March 14, 2012 from http://www.who.int/patientsafety/implementation/solutions/high5s/ps_medi....
-
- Gleason KM, McDaniel MR, Feinglass J, Baker DW, Lindquist L, Liss D, Noskin GA. Results of the medications at transitions and clinical handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25:441–447. doi: 10.1007/s11606-010-1256-6. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
