

Management of EGFR-inhibitor associated rash: a retrospective study in 49 patients
- PMID: 22472354
- PMCID: PMC3351712
- DOI: 10.1186/2047-783X-17-4
Management of EGFR-inhibitor associated rash: a retrospective study in 49 patients
Abstract
Background: In recent years inhibitors directed against the epidermal growth factor receptor (EGFR) have evolved as effective targeting cancer drugs. Characteristic papulopustular exanthemas, often described as acneiform rashes, are the most frequent adverse effect associated with this class of novel cancer drugs and develop in > 90% of patients. Notably, the rash may significantly compromise the patients' quality of life, thereby potentially leading to incompliance as well as dose reduction or even termination of the anti-EGFR therapy. Yet, an effective dermatologic management of cutaneous adverse effects can be achieved. Whereas various case reports, case series or expert opinions on the management of EGFR-inhibitor (EGFRI) induced rashes have been published, data on systematic management studies are sparse.
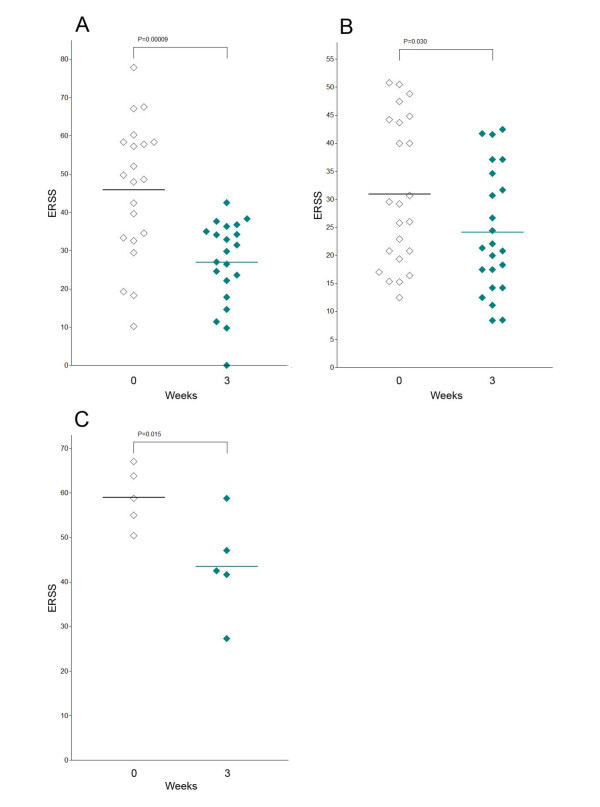
Methods: Here, we present a retrospective, uncontrolled, comparative study in 49 patients on three established regimens for the management of EGFRI-associated rashes.
Results: Strikingly, patients' rash severity improved significantly over three weeks of treatment with topical mometason furoate cream, topical prednicarbate cream plus nadifloxacin cream, as well as topical prednicarbate cream plus nadifloxacin cream plus systemic isotretinoin.
Conclusions: In summary our results demonstrate that EGFRI-associated rashes can be effectively managed by specific dermatologic interventions. Whereas mild to moderate rashes should be treated with basic measures in combination with topical glucocorticosteroids or combined regiments using glucocorticosteroids and antiseptics/antibiotics, more severe or therapy-resistant rashes are likely to respond with the addition of systemic retinoids.
Figures

Similar articles
-
Topical therapy with nadifloxacin cream and prednicarbate cream improves acneiform eruptions caused by the EGFR-inhibitor cetuximab - A report of 29 patients.Eur J Dermatol. 2010 Jan-Feb;20(1):82-4. doi: 10.1684/ejd.2010.0806. Epub 2009 Oct 2. Eur J Dermatol. 2010. PMID: 19797039 Clinical Trial.
-
Acneiform eruptions with combination targeted cancer therapy in colorectal cancer patients.Support Care Cancer. 2022 Oct;30(10):8051-8058. doi: 10.1007/s00520-022-07257-2. Epub 2022 Jun 30. Support Care Cancer. 2022. PMID: 35771289
-
Prophylactic Topical Treatment for EGFR Inhibitor-Induced Papulopustular Rash: A Randomized Clinical Trial.Dermatology. 2021;237(6):988-994. doi: 10.1159/000511869. Epub 2020 Dec 30. Dermatology. 2021. PMID: 33378750 Clinical Trial.
-
The extent to which the last decade has yielded additional treatment options for EGFR-associated rash besides classic treatment with antibiotics and corticosteroids - A systematic review.Eur J Oncol Nurs. 2021 Feb;50:101896. doi: 10.1016/j.ejon.2021.101896. Epub 2021 Jan 11. Eur J Oncol Nurs. 2021. PMID: 33493993
-
Skin toxicities associated with epidermal growth factor receptor inhibitors.Target Oncol. 2009 Apr;4(2):107-19. doi: 10.1007/s11523-009-0114-0. Epub 2009 May 19. Target Oncol. 2009. PMID: 19452131 Review.
Cited by
-
Management of human epidermal growth factor receptor inhibitors-related acneiform rash: A position paper based on the first Europe/USA Delphi consensus process.J Eur Acad Dermatol Venereol. 2025 Apr;39(4):730-741. doi: 10.1111/jdv.20391. Epub 2024 Oct 26. J Eur Acad Dermatol Venereol. 2025. PMID: 39460590 Free PMC article.
-
Adverse reactions to targeted and non-targeted chemotherapeutic drugs with emphasis on hypersensitivity responses and the invasive metastatic switch.Cancer Metastasis Rev. 2013 Dec;32(3-4):723-61. doi: 10.1007/s10555-013-9447-3. Cancer Metastasis Rev. 2013. PMID: 24043487 Free PMC article. Review.
-
Epidermal Growth Factor Receptor Inhibitor Skin Rash Prophylaxis in a Community Oncology Setting.J Adv Pract Oncol. 2018 Jul-Aug;9(5):489-495. Epub 2018 Jul 1. J Adv Pract Oncol. 2018. PMID: 31086685 Free PMC article. Review.
-
Updated Physician's Guide to the Off-label Uses of Oral Isotretinoin.J Clin Aesthet Dermatol. 2014 Apr;7(4):22-34. J Clin Aesthet Dermatol. 2014. PMID: 24765227 Free PMC article. Review.
-
[Cutaneous side effects of targeted cancer drugs].Hautarzt. 2017 Jan;68(1):12-18. doi: 10.1007/s00105-016-3902-3. Hautarzt. 2017. PMID: 27885401 Review. German.
References
-
- Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, Dummer R, Garbe C, Testori A, Maio M, Hogg D, Lorigan P, Lebbe C, Jouary T, Schadendorf D, Ribas A, O'Day SJ, Sosman JA, Kirkwood JM, Eggermont AM, Dreno B, Nolop K, Li J, Nelson B, Hou J, Lee RJ, Flaherty KT, McArthur GA. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Engl J Med. 2011;364:2507–2516. doi: 10.1056/NEJMoa1103782. - DOI - PMC - PubMed
-
- Gutzmer R, Becker JC, Enk A, Garbe C, Hauschild A, Leverkus M, Reimer G, Treudler R, Tsianakas A, Ulrich C, Wollenberg A, Homey B. Management of cutaneous side effects of EGFR inhibitors: recommendations from a German expert panel for the primary treating physician. J Dtsch Dermatol Ges. 2011;9:195–203. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
