

Decreased extra-renal urate excretion is a common cause of hyperuricemia
- PMID: 22473008
- PMCID: PMC3337984
- DOI: 10.1038/ncomms1756
Decreased extra-renal urate excretion is a common cause of hyperuricemia
Abstract
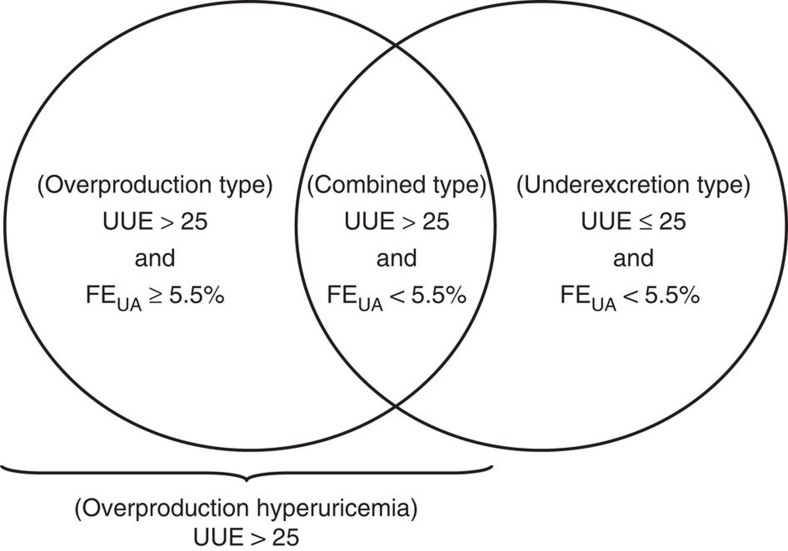
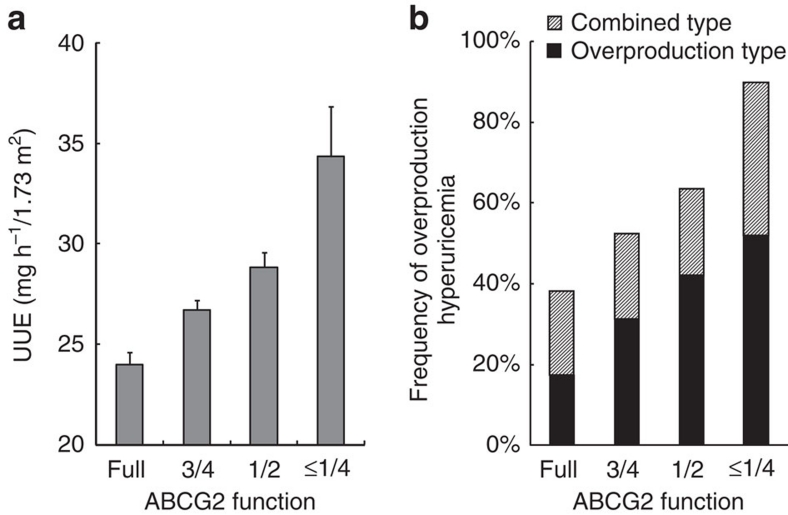
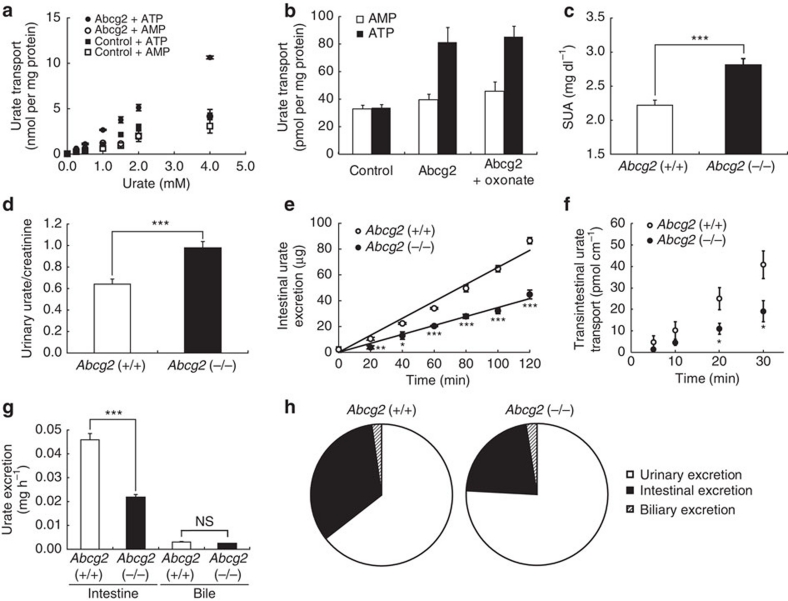
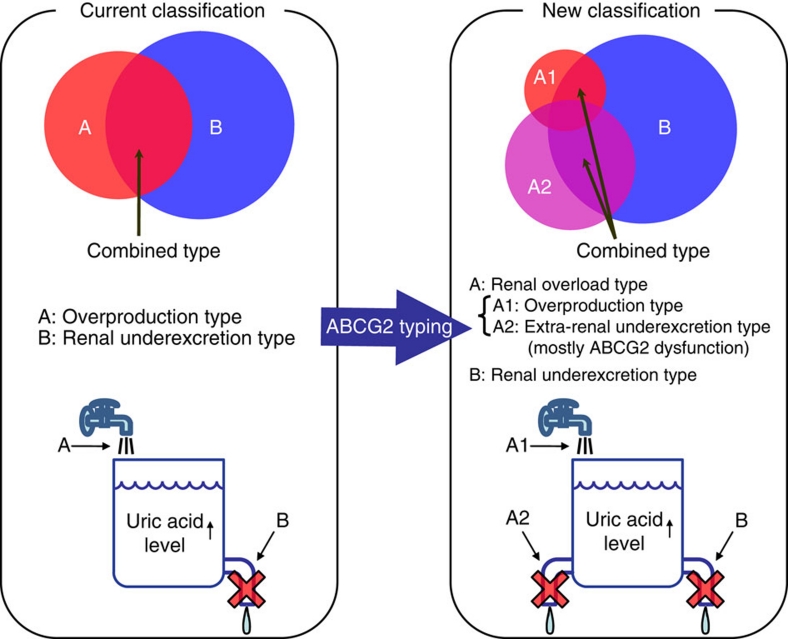
ABCG2, also known as BCRP, is a high-capacity urate exporter, the dysfunction of which raises gout/hyperuricemia risk. Generally, hyperuricemia has been classified into urate 'overproduction type' and/or 'underexcretion type' based solely on renal urate excretion, without considering an extra-renal pathway. Here we show that decreased extra-renal urate excretion caused by ABCG2 dysfunction is a common mechanism of hyperuricemia. Clinical parameters, including urinary urate excretion, are examined in 644 male outpatients with hyperuricemia. Paradoxically, ABCG2 export dysfunction significantly increases urinary urate excretion and risk ratio of urate overproduction. Abcg2-knockout mice show increased serum uric acid levels and renal urate excretion, and decreased intestinal urate excretion. Together with high ABCG2 expression in extra-renal tissues, our data suggest that the 'overproduction type' in the current concept of hyperuricemia be renamed 'renal overload type', which consists of two subtypes-'extra-renal urate underexcretion' and genuine 'urate overproduction'-providing a new concept valuable for the treatment of hyperuricemia and gout.
Figures
References
-
- Edwards N. L. The role of hyperuricemia in vascular disorders. Curr. Opin. Rheumatol. 21, 132–137 (2009). - PubMed
-
- Yeldandi A. V. et al.. Human urate oxidase gene: cloning and partial sequence analysis reveal a stop codon within the fifth exon. Biochem. Biophys. Res. Commun. 171, 641–646 (1990). - PubMed
-
- Sorensen L. B. Role of the intestinal tract in the elimination of uric acid. Arthritis Rheum. 8, 694–706 (1965). - PubMed
-
- Sica D. A. & Schoolwerth A. in Brenner and Rector's The Kidney (ed. B.M. Brenner) 645–649 (Saunders, 2004).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
