

Arterial calcification and bone physiology: role of the bone-vascular axis
- PMID: 22473330
- PMCID: PMC3423589
- DOI: 10.1038/nrendo.2012.36
Arterial calcification and bone physiology: role of the bone-vascular axis
Abstract
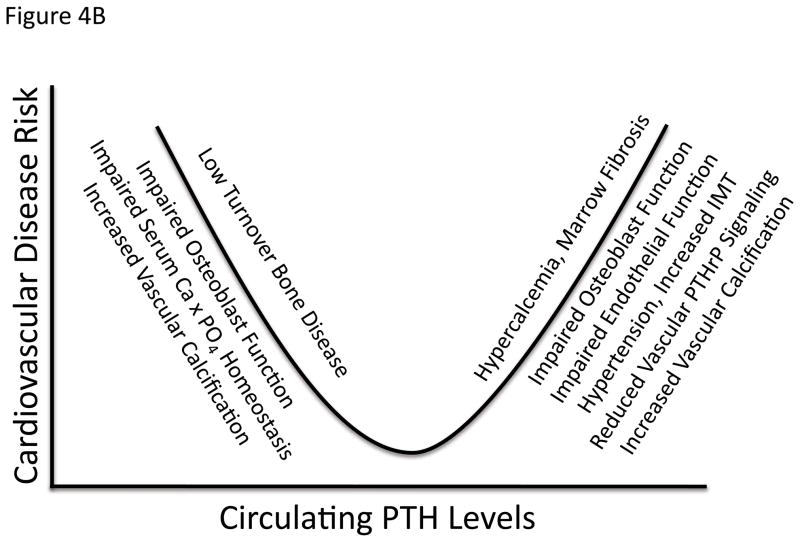
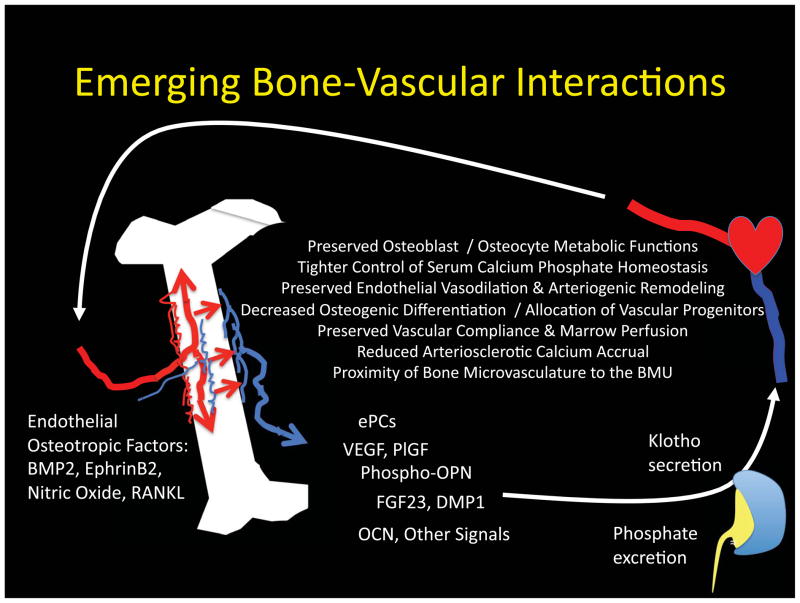
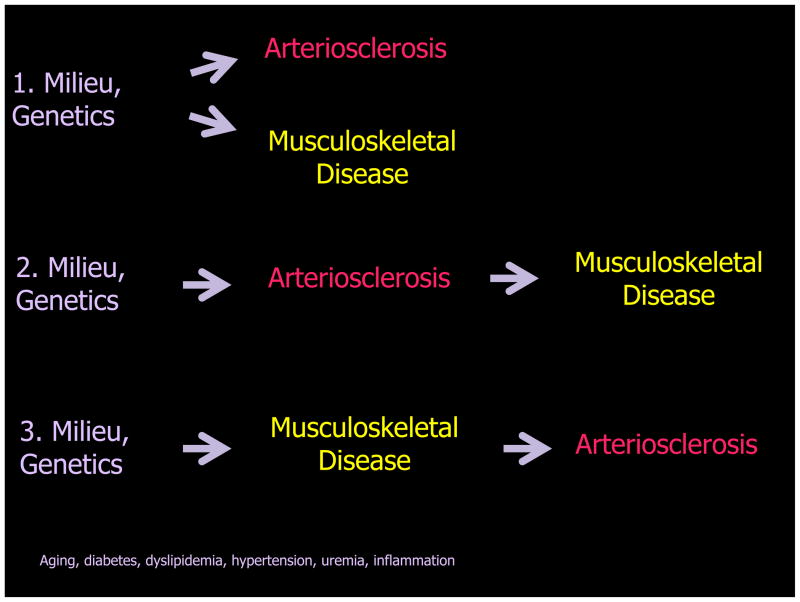
Bone never forms without vascular interactions. This simple statement of fact does not adequately reflect the physiological and pharmacological implications of the relationship. The vasculature is the conduit for nutrient exchange between bone and the rest of the body. The vasculature provides the sustentacular niche for development of osteoblast progenitors and is the conduit for egress of bone marrow cell products arising, in turn, from the osteoblast-dependent haematopoietic niche. Importantly, the second most calcified structure in humans after the skeleton is the vasculature. Once considered a passive process of dead and dying cells, vascular calcification has emerged as an actively regulated form of tissue biomineralization. Skeletal morphogens and osteochondrogenic transcription factors are expressed by cells within the vessel wall, which regulates the deposition of vascular calcium. Osteotropic hormones, including parathyroid hormone, regulate both vascular and skeletal mineralization. Cellular, endocrine and metabolic signals that flow bidirectionally between the vasculature and bone are necessary for both bone health and vascular health. Dysmetabolic states including diabetes mellitus, uraemia and hyperlipidaemia perturb the bone-vascular axis, giving rise to devastating vascular and skeletal disease. A detailed understanding of bone-vascular interactions is necessary to address the unmet clinical needs of an increasingly aged and dysmetabolic population.
Figures

References
-
- Zelzer E, et al. Skeletal defects in VEGF(120/120) mice reveal multiple roles for VEGF in skeletogenesis. Development. 2002;129:1893–904. - PubMed
-
- Qing H, et al. PTHR1 in Osteocytes Plays a Major role in Perilacunar Remodeling through the Activation of “Osteoclastic” Genes in Osteocytes. J Bone Miner Res. 2010;25(Suppl 1) Available at http://www.asbmr.org/Meetings/AnnualMeeting/AbstractDetail.aspx?aid=fbaf....
-
- Reeve J, et al. Skeletal blood flow, iliac histomorphometry, and strontium kinetics in osteoporosis: a relationship between blood flow and corrected apposition rate. J Clin Endocrinol Metab. 1988;66:1124–31. - PubMed
-
- Bianco P. Bone and the hematopoietic niche: a tale of two stem cells. Blood. 2011;117:5281–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
