

The value of anti-Mullerian hormone measurement in the long GnRH agonist protocol: association with ovarian response and gonadotrophin-dose adjustments
- PMID: 22473395
- PMCID: PMC3357198
- DOI: 10.1093/humrep/des101
The value of anti-Mullerian hormone measurement in the long GnRH agonist protocol: association with ovarian response and gonadotrophin-dose adjustments
Abstract
Background: This study evaluated the predictive value of serum and follicular fluid (FF) concentrations of anti-Müllerian hormone (AMH) with respect to treatment outcome variables in an IVF cycle.
Methods: A retrospective analysis was performed with data from 731 normogonadotrophic women undergoing controlled ovarian stimulation after stimulation with highly purified menotrophin (HP-hMG) or rFSH following a long GnRH agonist protocol.
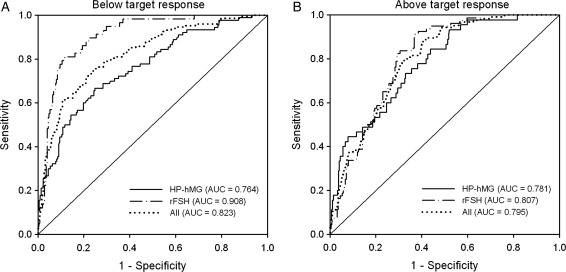
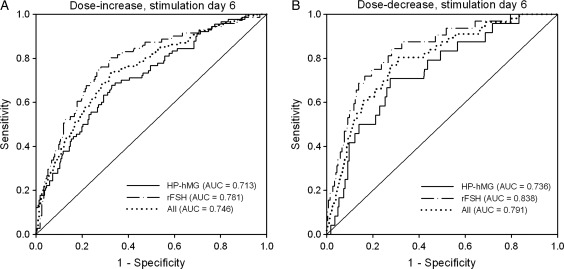
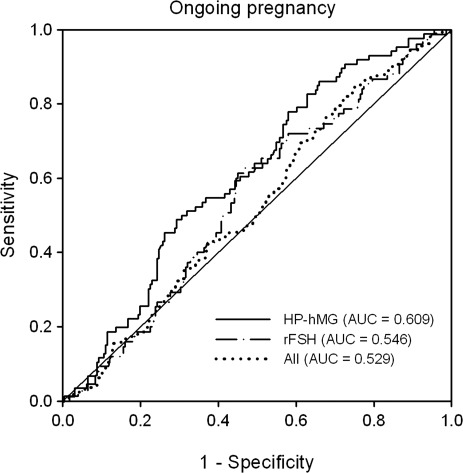
Results: In both treatment groups, the serum AMH concentration at the start of the stimulation was significantly (P < 0.001) positively correlated with the serum levels of estradiol (HP-hMG: r = 0.45; rFSH: r = 0.55), androstenedione (HP-hMG: r = 0.50; rFSH: 0.49) and total testosterone (HP-hMG: r = 0.40; rFSH: r = 0.36) at the end of the stimulation as well as the number of oocytes retrieved (HP-hMG: r = 0.48; rFSH: r = 0.62), the AMH concentration in FF (HP-hMG: r = 0.55; rFSH: 0.61) and the serum progesterone concentration (HP-hMG: r = 0.39; rFSH: r = 0.50) at oocyte retrieval. For both treatments, serum AMH at the start of the stimulation was a good predictor of the need to increase or decrease the gonadotrophin dose on stimulation day 6 and of ovarian response below (<7 oocytes) or above (>15 oocytes) the target. No significant relationships were observed between serum AMH and embryo quality or ongoing pregnancy.
Conclusion: The serum AMH concentration at the start of the stimulation in IVF patients down-regulated with GnRH agonist in the long protocol revealed a positive relationship with ovarian response to gonadotrophins in terms of oocytes retrieved and accompanying endocrine response. AMH is a good predictor of the need for gonadotrophin-dose adjustment on stimulation day 6 for patients with a fixed starting dose, but a poor predictor of embryo quality and pregnancy chances in individual patients.
Figures
References
-
- Arce J-C, Nyboe Andersen A, Collins J. Resolving methodological and clinical issues in the design of efficacy trials in assisted reproductive technologies: a mini-review. Hum Reprod. 2005;20:1757–1771. doi:10.1210/en.136.11.4951. - DOI - PubMed
-
- Baarends WM, Uilenbroek JT, Kramer P, Hoogerbrugge JW, van Leeuwen EC, Themmen AP, Grootegoed JA. Anti-mullerian hormone and anti-mullerian hormone type II receptor messenger ribonucleic acid expression in rat ovaries during postnatal development, the estrous cycle, and gonadotropin-induced follicle growth. Endocrinology. 1995;136:4951–4962. doi:10.1210/en.136.11.4951. - DOI - PubMed
-
- Broer SL, Mol BW, Hendriks D, Broekmans FJ. The role of antimullerian hormone in prediction of outcome after IVF: comparison with the antral follicle count. Fertil Steril. 2009;91:705–714. doi:10.1016/j.fertnstert.2007.12.013. - DOI - PubMed
-
- Broer SL, Mol B, Dólleman M, Fauser BC, Broekmans FJ. The role of anti-Müllerian hormone assessment in assisted reproductive technology outcome. Curr Opin Obstet Gynecol. 2010;22:193–201. doi:10.1097/GCO.0b013e3283384911. - DOI - PubMed
-
- Broer SL, Dólleman M, Opmeer BC, Fauser BC, Mol BW, Broekmans FJ. AMH and AFC as predictors of excessive response in controlled ovarian hyperstimulation: a meta-analysis. Hum Reprod Update. 2011;17:46–54. doi:10.1093/humupd/dmq034. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
