

Patterns of care at end of life in children with advanced heart disease
- PMID: 22473887
- PMCID: PMC4119813
- DOI: 10.1001/archpediatrics.2011.1829
Patterns of care at end of life in children with advanced heart disease
Abstract
Objective: To describe patterns of care for pediatric patients with advanced heart disease who experience in-hospital death.
Design: Retrospective single-institution medical record review.
Setting: A tertiary care pediatric hospital.
Participants: All patients younger than 21 years who died in the inpatient setting between January 1, 2007, and December 31, 2009, with primary cardiac diagnoses or who had ever received a cardiology consult (N=468). After excluding patients with significant noncardiac primary diagnoses, 111 children formed the analytic sample.
Main outcome measure: In-hospital deaths of children with heart disease during a 3-year period.
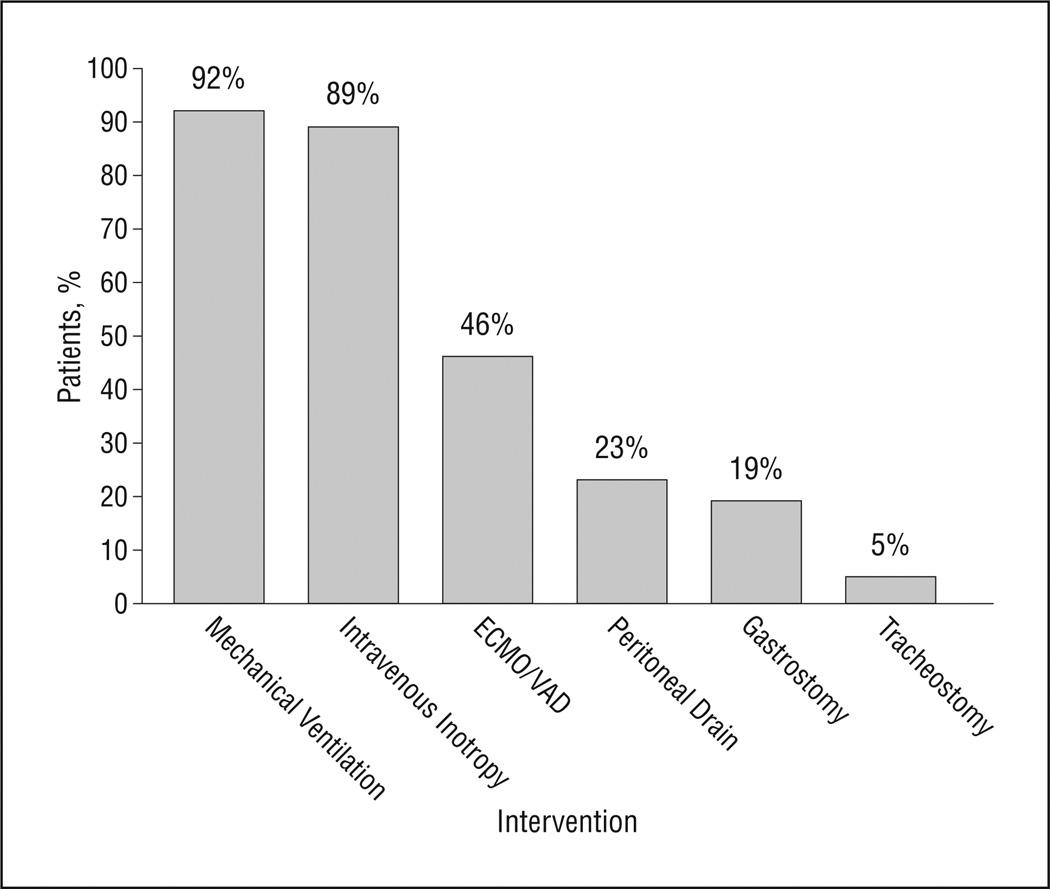
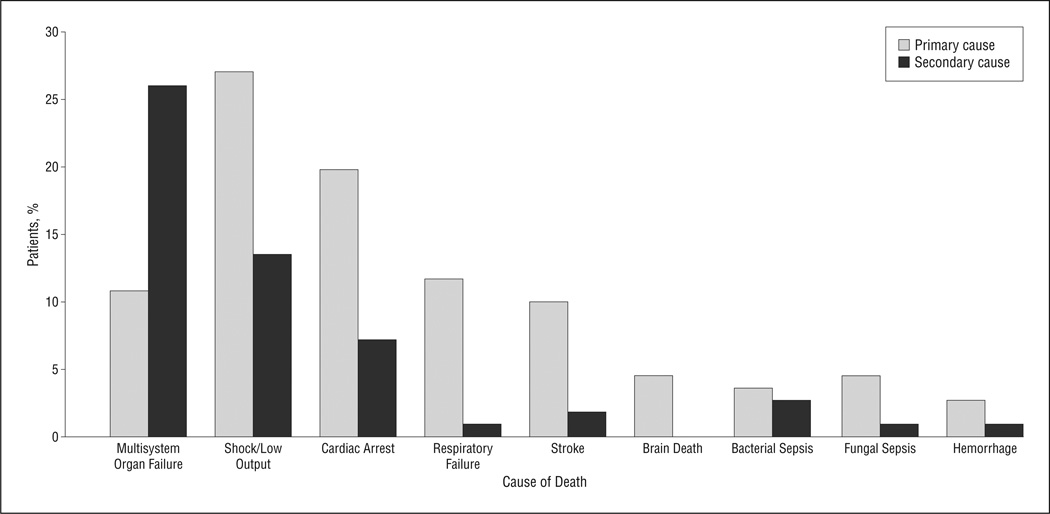
Results: Median age at death was 4.8 months (age range,1 day to 20.5 years), with 84 deaths (75.7%) occurring before age 1 year. Median length of terminal hospital stay was 22 days (range, 1-199 days). Diagnoses included 84 patients (75.7%) with congenital heart disease, 10 (9.0%)with cardiomyopathy/myocarditis, 9 (8.1%) with pulmonary hypertension, and 8 (7.2%) with heart transplants.Sixty-two patients (55.9%) had received cardio-pulmonary resuscitation during their last hospital admission. At the end of life, 21 children (18.9%) had gastrostomy tubes and 26 (23.4%) had peritoneal drains.Most patients (91.9%) received ventilation, with half also receiving mechanical circulatory support. Eighty-three patients (74.8%) experienced additional end-organ failure. Classified by mode of death, 76 patients (68.5%) had disease-directed support withdrawn, 28 (25.2%) died during resuscitation, and 7 (6.3%) died while receiving comfort care after birth. Eighty-three percent of parents were present at the time of death.
Conclusion: Infants and children who die of advanced heart disease frequently succumb in the intensive care setting with multisystem organ failure and exposure to highly technical care.
Figures
Comment in
-
Expanding the envelope of care.Arch Pediatr Adolesc Med. 2012 Aug;166(8):772-3. doi: 10.1001/archpediatrics.2012.150. Arch Pediatr Adolesc Med. 2012. PMID: 22473886 No abstract available.
References
-
- Boneva RS, Botto LD, Moore CA, Yang Q, Correa A, Erickson JD. Mortality associated with congenital heart defects in the United States: trends and racial disparities, 1979–1997. Circulation. 2001;103(19):2376–2381. - PubMed
-
- Heron M, Sutton PD, Xu J, Ventura SJ, Strobino DM, Guyer B. Annual summary of vital statistics: 2007. Pediatrics. 2010;125(1):4–15. - PubMed
-
- Rosenthal D, Chrisant MR, Edens E, et al. International Society for Heart and Lung Transplantation: practice guidelines for management of heart failure in children. J Heart Lung Transplant. 2004;23(12):1313–1333. - PubMed
-
- Ullrich CK, Dussel V, Hilden JM, Sheaffer JW, Lehmann L, Wolfe J. End-of-life experience of children undergoing stem cell transplantation for malignancy: parent and provider perspectives and patterns of care. Blood. 2010;115(19):3879–3885. - PubMed
