

Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk
- PMID: 22474203
- PMCID: PMC3891886
- DOI: 10.1001/jama.2012.388
Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk
Abstract
Context: Annual ultrasound screening may detect small, node-negative breast cancers that are not seen on mammography. Magnetic resonance imaging (MRI) may reveal additional breast cancers missed by both mammography and ultrasound screening.
Objective: To determine supplemental cancer detection yield of ultrasound and MRI in women at elevated risk for breast cancer.
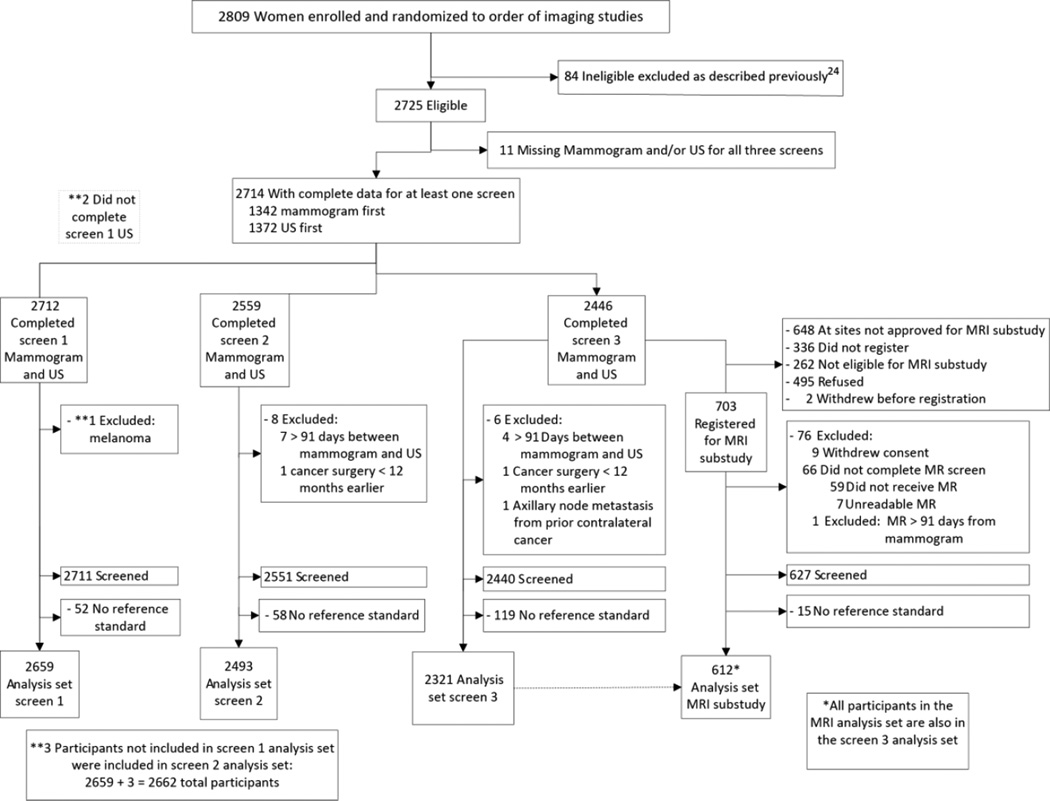
Design, setting, and participants: From April 2004-February 2006, 2809 women at 21 sites with elevated cancer risk and dense breasts consented to 3 annual independent screens with mammography and ultrasound in randomized order. After 3 rounds of both screenings, 612 of 703 women who chose to undergo an MRI had complete data. The reference standard was defined as a combination of pathology (biopsy results that showed in situ or infiltrating ductal carcinoma or infiltrating lobular carcinoma in the breast or axillary lymph nodes) and 12-month follow-up.
Main outcome measures: Cancer detection rate (yield), sensitivity, specificity, positive predictive value (PPV3) of biopsies performed and interval cancer rate.
Results: A total of 2662 women underwent 7473 mammogram and ultrasound screenings, 110 of whom had 111 breast cancer events: 33 detected by mammography only, 32 by ultrasound only, 26 by both, and 9 by MRI after mammography plus ultrasound; 11 were not detected by any imaging screen. Among 4814 incidence screens in the second and third years combined, 75 women were diagnosed with cancer. Supplemental incidence-screening ultrasound identified 3.7 cancers per 1000 screens (95% CI, 2.1-5.8; P < .001). Sensitivity for mammography plus ultrasound was 0.76 (95% CI, 0.65-0.85); specificity, 0.84 (95% CI, 0.83-0.85); and PPV3, 0.16 (95% CI, 0.12-0.21). For mammography alone, sensitivity was 0.52 (95% CI, 0.40-0.64); specificity, 0.91 (95% CI, 0.90-0.92); and PPV3, 0.38 (95% CI, 0.28-0.49; P < .001 all comparisons). Of the MRI participants, 16 women (2.6%) had breast cancer diagnosed. The supplemental yield of MRI was 14.7 per 1000 (95% CI, 3.5-25.9; P = .004). Sensitivity for MRI and mammography plus ultrasound was 1.00 (95% CI, 0.79-1.00); specificity, 0.65 (95% CI, 0.61-0.69); and PPV3, 0.19 (95% CI, 0.11-0.29). For mammography and ultrasound, sensitivity was 0.44 (95% CI, 0.20-0.70, P = .004); specificity 0.84 (95% CI, 0.81-0.87; P < .001); and PPV3, 0.18 (95% CI, 0.08 to 0.34; P = .98). The number of screens needed to detect 1 cancer was 127 (95% CI, 99-167) for mammography; 234 (95% CI, 173-345) for supplemental ultrasound; and 68 (95% CI, 39-286) for MRI after negative mammography and ultrasound results.
Conclusion: The addition of screening ultrasound or MRI to mammography in women at increased risk of breast cancer resulted in not only a higher cancer detection yield but also an increase in false-positive findings.
Trial registration: clinicaltrials.gov Identifier: NCT00072501.
Figures
Comment in
-
Supplementary imaging for breast cancer screening in high-risk women.JAMA. 2012 Jul 18;308(3):236; author reply 236-7. doi: 10.1001/jama.2012.7545. JAMA. 2012. PMID: 22797633 No abstract available.
-
Supplementary imaging for breast cancer screening in high-risk women.JAMA. 2012 Jul 18;308(3):236; author reply 236-7. doi: 10.1001/jama.2012.7547. JAMA. 2012. PMID: 22797634 No abstract available.
References
-
- Buchberger W, Niehoff A, Obrist P, DeKoekkoek-Doll P, Dunser M. Clinically and mammographically occult breast lesions: detection and classification with high-resolution sonography. Semin Ultrasound CT MR. 2000;21(4):325–336. - PubMed
-
- Crystal P, Strano SD, Shcharynski S, Koretz MJ. Using sonography to screen women with mammographically dense breasts. AJR Am J Roentgenol. 2003 Jul;181(1):177–182. - PubMed
-
- Gordon PB, Goldenberg SL. Malignant breast masses detected only by ultrasound. A retrospective review [see comments] Cancer. 1995;76(4):626–630. - PubMed
-
- Kaplan SS. Clinical utility of bilateral whole-breast US in the evaluation of women with dense breast tissue. Radiology. 2001 Dec;221(3):641–649. - PubMed
-
- Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: An analysis of 27,825 patient evaluations. Radiology. 2002 Oct;225(1):165–175. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
