

Reconstruction by Pancreaticogastrostomy versus Pancreaticojejunostomy following Pancreaticoduodenectomy: A Meta-Analysis of Randomized Controlled Trials
- PMID: 22474444
- PMCID: PMC3296445
- DOI: 10.1155/2012/627095
Reconstruction by Pancreaticogastrostomy versus Pancreaticojejunostomy following Pancreaticoduodenectomy: A Meta-Analysis of Randomized Controlled Trials
Abstract
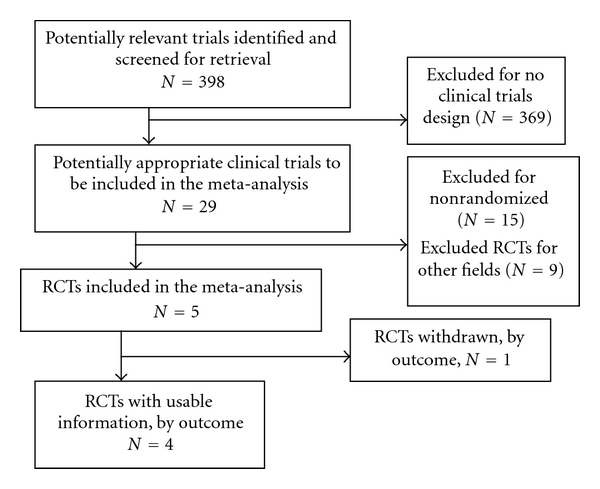
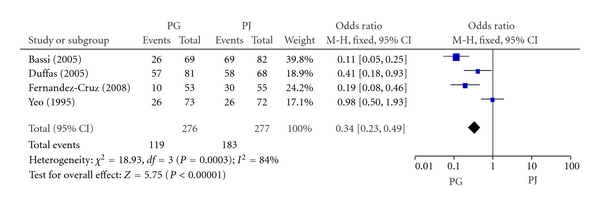
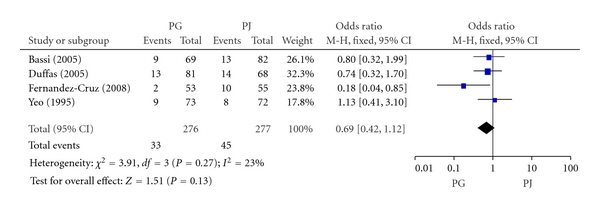
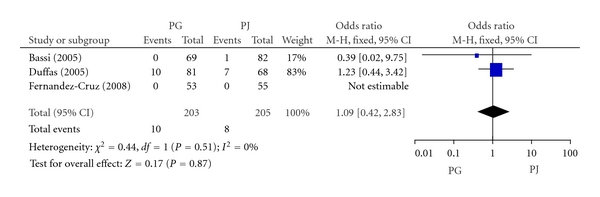
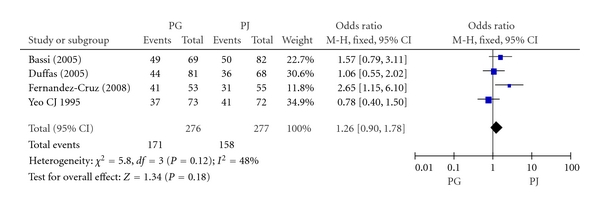
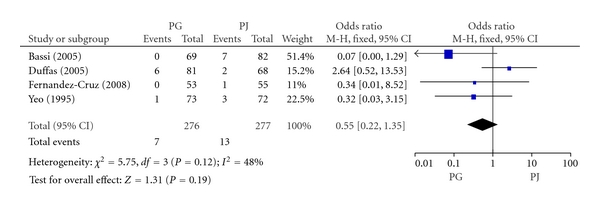
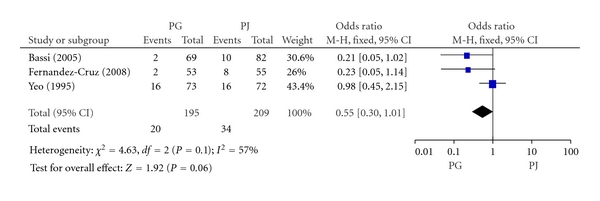
Objectives. The aim of our study was to evaluate and compare the results of pancreaticogastrostomy (PG) and pancreaticojejunostomy (PJ) after pancreaticoduodenectomy (PD). Methods. Published data of randomized clinical trials (RCTs) comparing the clinically relevant outcomes of PG versus PJ after PD were analyzed. Two reviewers assessed the quality of each trial and collected data independently. The Cochrane Collaboration's RevMan 5.0 software was used for statistical analysis. Proportions were combined, and the odds ratio (OR) with its 95% CI was used as the effect size estimate. Results. Four RCTs published in 1995 or later were included in this meta-analysis, in which 276 patients underwent PG and 277 patients underwent PJ followed PD. In the combined results of PG versus PJ, a significant difference in the morbidity of intra-abdominal complications (OR, 0.34; 95% CI, 0.23-0.49; P < 0.00001) was found, but no significant difference could be found for pancreatic fistula (OR, 0.69; 95% CI, 0.42-1.12 , P = 0.13) mortality (OR, 1.09; 95% CI, 0.42-2.83; P = 0.87), recovery with no complications (OR, 1.26; 95% CI, 0.90-1.78; P = 0.18), biliary fistula (OR, 0.55; 95% CI, 0.22-1.35; P = 0.19), or in delayed gastric emptying (OR, 0.55; 95% CI, 0.33-1.01; P = 0.06). Conclusions. Current RCTs suggest that PG is better than PJ for pancreatic reconstruction after PD.
Figures
References
-
- Shrikhande SV, Qureshi SS, Rajneesh N, Shukla PJ. Pancreatic anastomoses after pancreaticoduodenectomy: do we need further studies? World Journal of Surgery. 2005;29(12):1642–1649. - PubMed
-
- Winter JM, Cameron JL, Campbell KA, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. Journal of Gastrointestinal Surgery. 2006;10(9):1199–1211. - PubMed
LinkOut - more resources
Full Text Sources
