

doi: 10.5402/2012/456706.
Epub 2012 Mar 11.
18-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Management of Aggressive Non-Hodgkin's B-Cell Lymphoma
Affiliations
- PMID: 22474590
- PMCID: PMC3313577
- DOI: 10.5402/2012/456706
Item in Clipboard
18-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Management of Aggressive Non-Hodgkin's B-Cell Lymphoma
ISRN Hematol.
2012.
Abstract
18-Fluorodeoxyglucose (FDG-PET/CT) is an established imaging modality that has been proven to be of benefit in the management of aggressive B-cell non-Hodgkin's lymphoma, such as diffuse large B-cell lymphoma and advanced stage follicular lymphoma. The combination of anatomic and functional imaging afforded by FDG-PET/CT has led to superior sensitivity and specificity in the primary staging, restaging, and assessment of response to treatment of hematological malignancies when compared to FDG-PET and CT alone. The use of FDG-PET/CT for posttreatment surveillance imaging remains controversial, and further study is needed to ascertain whether this modality is cost effective and appropriate for use in this setting.
Figures
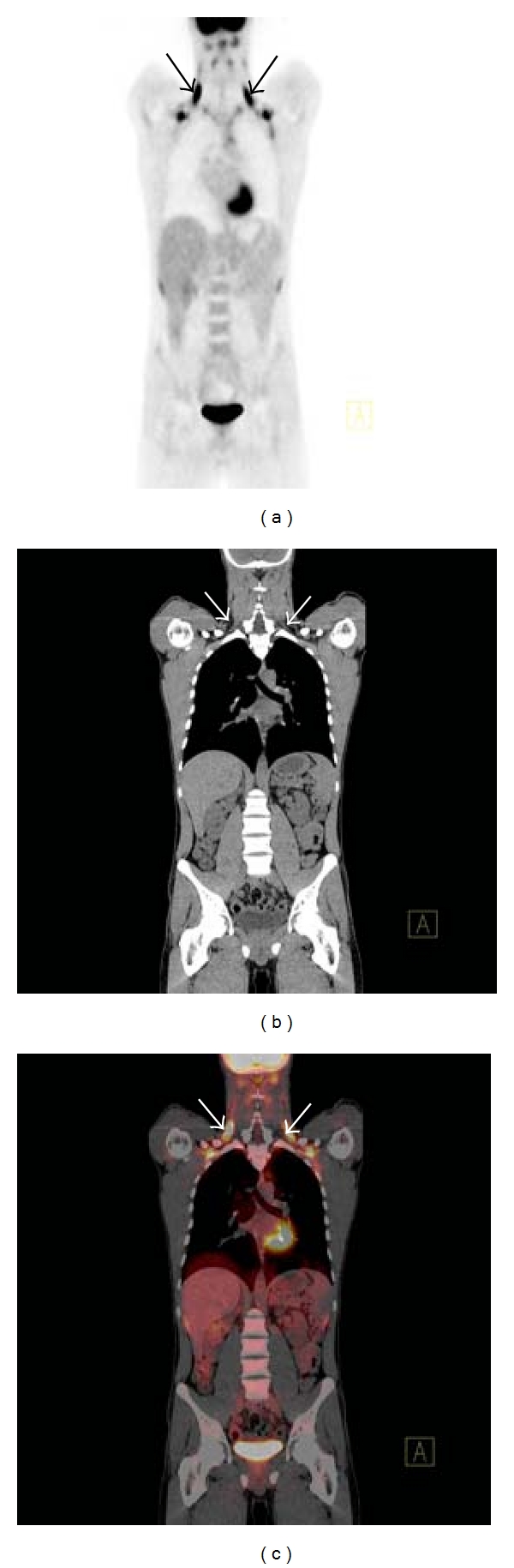
Coronal PET maximum intensity projection (MIP) image (a) displaying foci of increased radiotracer uptake bilaterally in the neck in a patient with treated DLBSL. The corresponding coronal CT (b) and fused FDG-PET/CT (c) demonstrate no abnormality and the areas with increased FDG uptake correspond to regions of fat density (arrows). This is the characteristic appearance of hypermetabolic brown fat on FDG-PET/CT.
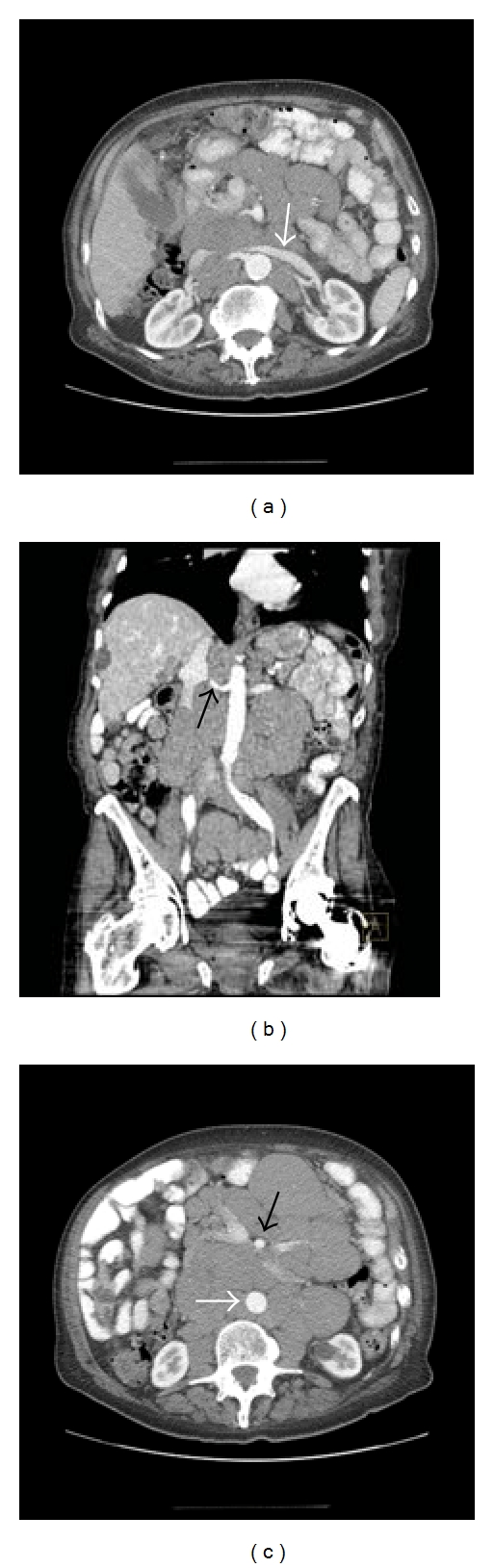
Axial (a) and coronal (b) contrast enhanced CT of the abdomen in a patient with chronic lymphocytic leukemia displaying encasement of vessels such as the left renal vein (white arrow) and right renal artery (black arrow) by lymph nodes masses, the so-called “sandwich sign.” Axial contrast enhanced CT (c) of the abdomen at a lower level in the same patient displaying elevation of the abdominal aorta off the vertebral column (white arrow) which is a characteristic feature of lymphoma and helps to differentiate lymphoma from other retroperitoneal masses, such as retroperitoneal fibrosis. Note the encasement of the superior mesenteric artery (SMA) by the lymph node mass and increased separation of the SMA from the aorta (black arrow).
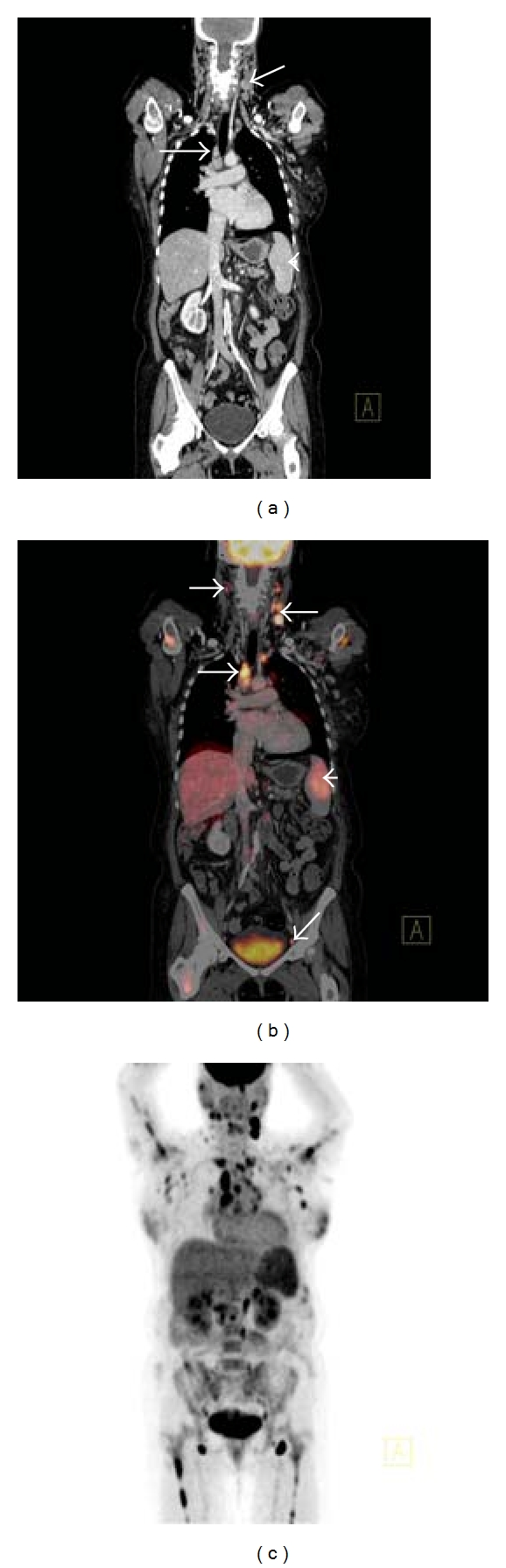
Coronal CT (a) demonstrating left cervical and right paratracheal lymphadenopathy (white arrows) and mild splenomegaly (white arrowhead) consistent with high-grade follicular lymphoma. Corresponding coronal fused FDG-PET/CT (b) demonstrates increased radiotracer uptake in the pathologically enlarged left cervical and right paratracheal lymphadenopathy (white arrows) and spleen (white arrowhead), but also abnormal FDG accumulation in right cervical and left external iliac lymph nodes (white arrows) that appeared normal by size criteria on the corresponding CT scan. Coronal PET MIP (c) in the same patient demonstrating widespread increased radiotracer uptake throughout the neck, thorax, abdomen, and proximal humeri and femora bilaterally; the widespread bone marrow involvement was not apparent on CT.
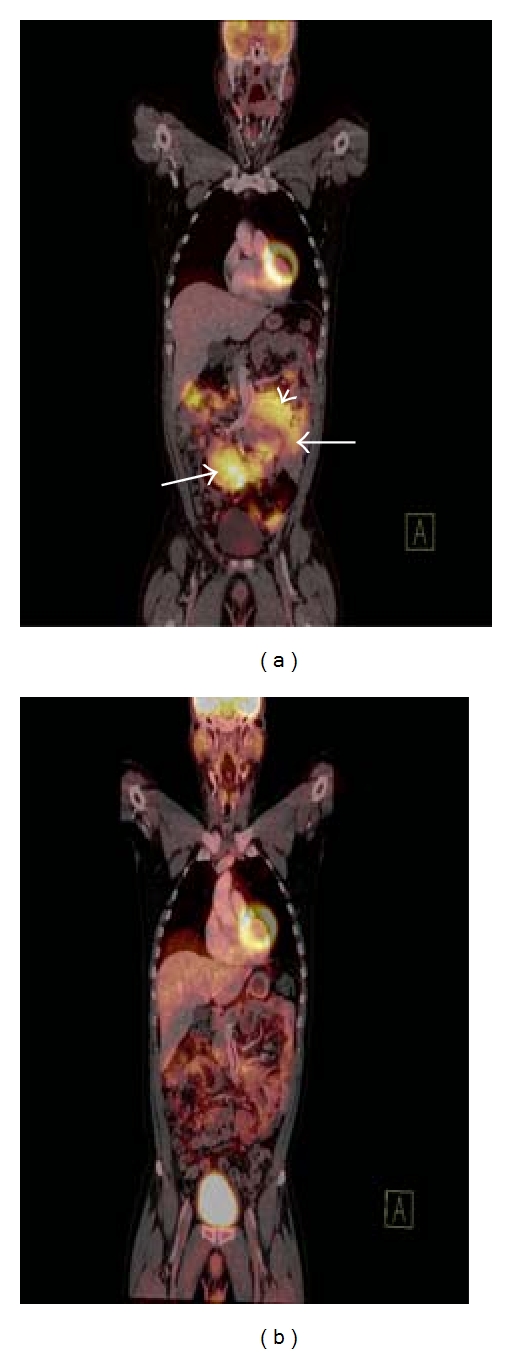
Coronal fused FDG-PET/CT image (a) demonstrating increased radiotracer uptake in multiple intra-abdominal lymph node masses in a patient with DLBCL (white arrows). Note how a large soft tissue mass displaces the small bowel and the mesenteric vessels (white arrowhead). Coronal fused FDG-PET/CT image (b) in the same patient demonstrating complete resolution of the previously described soft tissue masses. The observed residual FDG avidity is within bowel and is normal. This FDG-PET/CT confirms complete response to treatment.
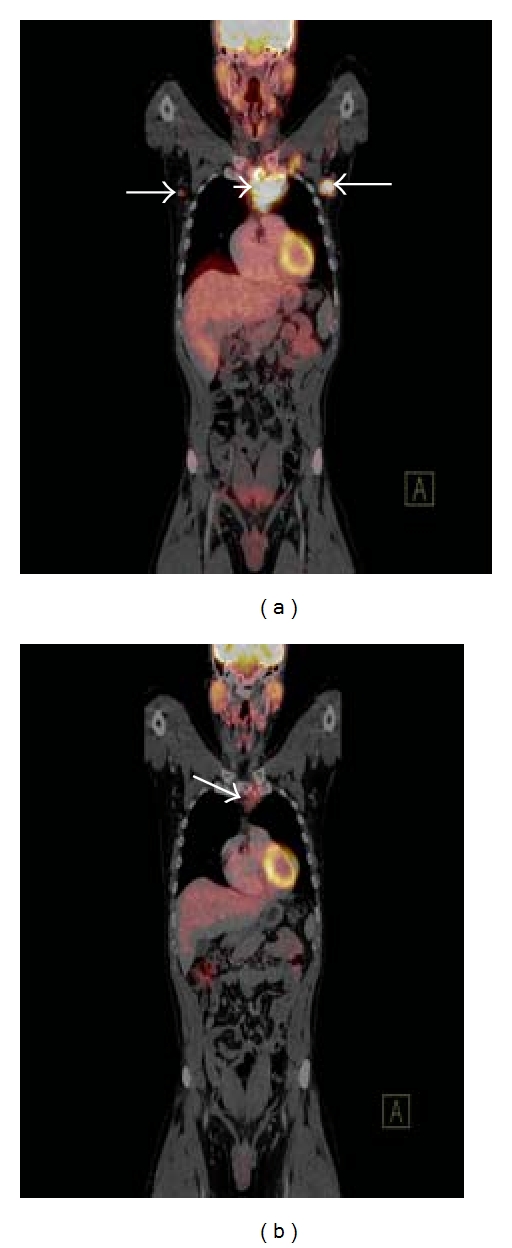
Coronal fused FDG-PET/CT image (a) of a patient with nodular sclerosis type Hodgkin's lymphoma prechemotherapy demonstrating an FDG-avid lymph node mass in the superior mediastinum (white arrowhead) and hypermetabolic bilateral axillary lymphadenopathy (white arrows). Interim staging coronal fused FDG-PET/CT image (b) in the same patient after 3 cycles of chemotherapy demonstrating a significant interval decrease in both the degree of FDG uptake and the size of the lymph node mass in the superior mediastinum (white arrow) with resolution of the axillary lymphadenopathy.
Similar articles
-
Different roles of surveillance positron emission tomography according to the histologic subtype of non-Hodgkin's lymphoma.Korean J Intern Med. 2021 Mar;36(Suppl 1):S245-S252. doi: 10.3904/kjim.2019.376. Epub 2020 Jun 19. Korean J Intern Med. 2021. PMID: 32550718 Free PMC article.
-
Frequent impact of [18F]fluorodeoxyglucose positron emission tomography on the staging and management of patients with indolent non-Hodgkin's lymphoma.Clin Lymphoma. 2003 Jun;4(1):43-9. doi: 10.3816/clm.2003.n.013. Clin Lymphoma. 2003. PMID: 12837154
-
Whole-body positron emission tomography using 18F-fluorodeoxyglucose for posttreatment evaluation in Hodgkin's disease and non-Hodgkin's lymphoma has higher diagnostic and prognostic value than classical computed tomography scan imaging.Blood. 1999 Jul 15;94(2):429-33. Blood. 1999. PMID: 10397709
-
The role of 18F-FDG PET and 18F-FDG PET/CT in the evaluation of pediatric Hodgkin's lymphoma and non-Hodgkin's lymphoma.Hell J Nucl Med. 2013 Sep-Dec;16(3):230-6. doi: 10.1967/s0024499100091. Epub 2013 Oct 2. Hell J Nucl Med. 2013. PMID: 24137577 Review.
-
[The role of PET/CT investigation in the management of patients with diffuse large B-cell lymphoma].Magy Onkol. 2016 Jun 6;60(2):108-17. Epub 2016 Mar 23. Magy Onkol. 2016. PMID: 27275637 Review. Hungarian.
Cited by
-
Screening of trace elements in hair of the female population with different types of cancers in Wielkopolska region of Poland.ScientificWorldJournal. 2014;2014:953181. doi: 10.1155/2014/953181. Epub 2014 Dec 15. ScientificWorldJournal. 2014. PMID: 25580464 Free PMC article.
-
[¹⁸F]fluoro-2-deoxy-d-glucose positron emission tomography/computed tomography imaging in oncology: initial staging and evaluation of cancer therapy.Med Princ Pract. 2013;22(5):427-37. doi: 10.1159/000346303. Epub 2013 Jan 26. Med Princ Pract. 2013. PMID: 23363934 Free PMC article. Review.
-
Specialized second-opinion radiology review of PET/CT examinations for patients with diffuse large B-cell lymphoma impacts patient care and management.Medicine (Baltimore). 2017 Dec;96(51):e9411. doi: 10.1097/MD.0000000000009411. Medicine (Baltimore). 2017. PMID: 29390562 Free PMC article.
References
-
- Flowers CR, Armitage JO. A decade of progress in lymphoma: advances and continuing challenges. Clinical Lymphoma, Myeloma and Leukemia. 2010;10(6):414–423. - PubMed
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer Journal for Clinicians. 2010;60(5):277–300. - PubMed
-
- Cronin CG, Swords R, Truong MT, et al. Clinical utility of PET/CT in lymphoma. American Journal of Roentgenology. 2010;194(1):W91–W103. - PubMed
LinkOut - more resources
Full Text Sources