

Experience of Advate rAHF-PFM in previously untreated patients and minimally treated patients with haemophilia A
- PMID: 22476554
- PMCID: PMC6292131
- DOI: 10.1160/TH11-09-0642
Experience of Advate rAHF-PFM in previously untreated patients and minimally treated patients with haemophilia A
Abstract
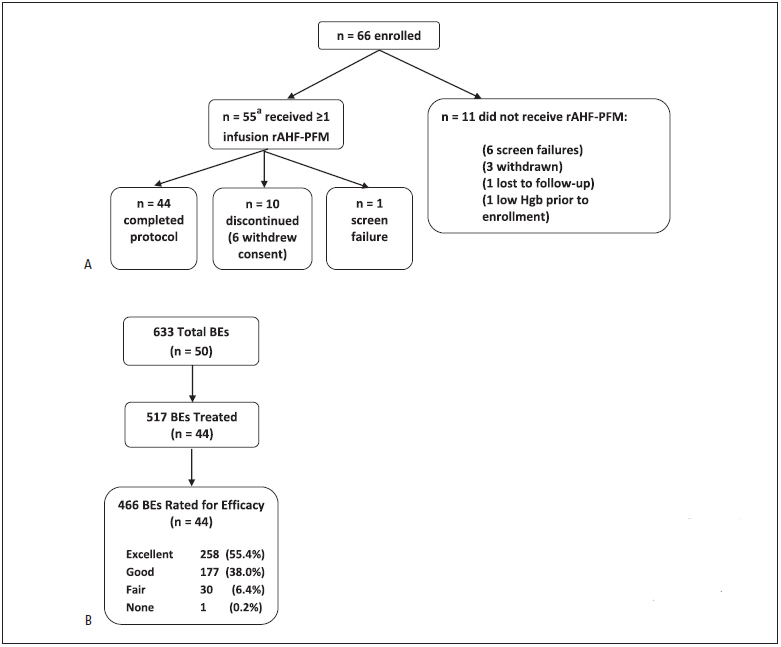
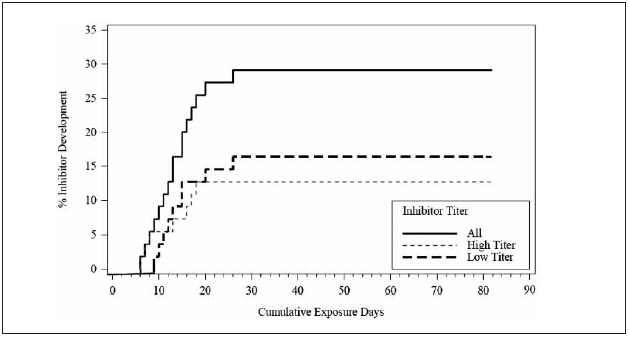
We report a prospective trial of 55 previously untreated patients (PUPs) and minimally treated patients (MTPs) with severe/moderately severe haemophilia A (baseline factor VIII [FVIII] ≤2%) treated with a single FVIII replacement product. It was the objective of this study to evaluate the immunogenicity, efficacy, and safety of rAHF-PFM (Advate®). On-demand or prophylactic treatment regimens were determined at the discretion of the investigator. rAHF-PFM was also permitted for perioperative management. There were 633 bleeding episodes (BEs), including 517 treated, and 466 rated for efficacy. Haemostatic efficacy was considered excellent/good in 93% of 466 rated treatments. Of 517 treated BEs, 463/517 (90%) were managed with one (356/517 [69%]) or two infusions (107/517 [21%]). There were 27 surgeries. Intraoperative (n=22) and postoperative (n=25) haemostatic efficacies were considered excellent or good in 100% of rated surgeries. Related serious adverse events (SAEs) were inhibitor development in 16/55 (29.1%) subjects who received at least one infusion of rAHF-PFM. Non-serious, related adverse events (AEs) were few in number (14 in eight subjects). The odds ratio (OR [95% Confidence Interval, CI]) of developing inhibitors was significantly higher in subjects with a family history of inhibitor (4.95[1.29-19.06]), non-Caucasian ethnicity (4.18, [1.18-14.82]), and intensive treatment at high dose (4.5 [1.05-19.25]) within ≤20 exposure days (EDs). In conclusion, rAHF-PFM was safe and effective for the management and perioperative coverage of PUPs/MTPs with severe/moderately severe haemophilia A. This report supports previous findings from studies in which family history of inhibitor, non-Caucasian ethnicity, and high intensity treatment were associated with high risk of inhibitor development.
Trial registration: ClinicalTrials.gov NCT00157157.
Conflict of interest statement
Figures
References
-
- Tarantino MD, Collins PW, Hay CR et al. Clinical evaluation of an advanced category antihaemophilic factor prepared using a plasma/albumin-free method: pharmacokinetics, efficacy, and safety in previously treated patients with haemophilia A. Haemophilia. 2004;10:428–437. - PubMed
-
- Blanchette VS, Shapiro AD, Liesner RJ et al. Plasma and albumin free recombinant factor VIII (rAHF-PFM): pharmacokinetics, efficacy and safety in previously treated pediatric patients. J Thromb Haemost. 2008;6:1319–1326. - PubMed
-
- Negrier C, Shapiro A, Berntorp E et al. Surgical evaluation of a recombinant Factor VIII prepared using a plasma/albumin-free method: Efficacy and safety of Advate in previously treated patients. Thromb Haemost. 2008;100:217–223. - PubMed
-
- Franchini M, Tagliaferri A, Mengoli C et al. Cumulative inhibitor incidence in previously untreated patients with severe hemophilia A treated with plasma-derived versus recombinant factor VIII concentrates: A critical systematic review. Crit Rev Oncol Hematol. 2012;81:82–93. - PubMed
-
- Iorio A, Halimeh S, Holzhauer S et al. Rate of inhibitor development in previously untreated hemophilia A patients treated with plasma-derived or recombinant factor VIII concentrates: a systematic review. J Thromb Haemost. 2010;8:1256–1265. - PubMed