

Additional diverse findings expand the clinical presentation of DOCK8 deficiency
- PMID: 22476911
- PMCID: PMC3732775
- DOI: 10.1007/s10875-012-9664-5
Additional diverse findings expand the clinical presentation of DOCK8 deficiency
Abstract
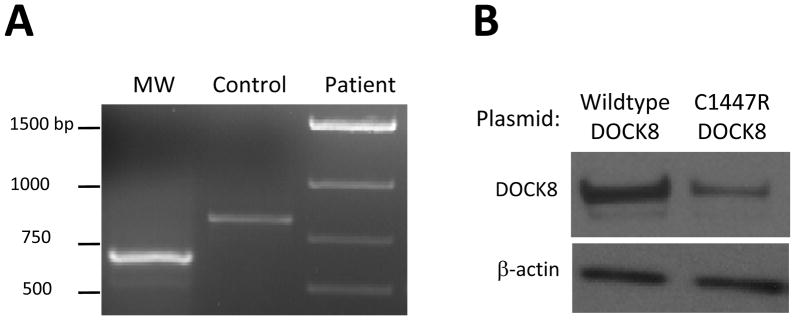
We describe seven Turkish children with DOCK8 deficiency who have not been previously reported. Three patients presented with typical features of recurrent or severe cutaneous viral infections, atopic dermatitis, and recurrent respiratory or gastrointestinal tract infections. However, four patients presented with other features. Patient 1-1 featured sclerosing cholangitis and colitis; patient 2-1, granulomatous soft tissue lesion and central nervous system involvement, with primary central nervous system lymphoma found on follow-up; patient 3-1, a fatal metastatic leiomyosarcoma; and patient 4-2 showed no other symptoms initially besides atopic dermatitis. Similar to other previously reported Turkish patients, but in contrast to patients of non-Turkish ethnicity, the patients' lymphopenia was primarily restricted to CD4(+) T cells. Patients had homozygous mutations in DOCK8 that altered splicing, introduced premature terminations, destabilized protein, or involved large deletions within the gene. Genotyping of remaining family members showed that DOCK8 deficiency is a fully penetrant, autosomal recessive disease. In our patients, bone marrow transplantation resulted in rapid improvement followed by disappearance of viral skin lesions, including lesions resembling epidermodysplasia verruciformis, atopic dermatitis, and recurrent infections. Particularly for patients who feature unusual clinical manifestations, immunological testing, in conjunction with genetic testing, can prove invaluable in diagnosing DOCK8 deficiency and providing potentially curative treatment.
Figures




Similar articles
-
Cutaneous manifestations of DOCK8 deficiency syndrome.Arch Dermatol. 2012 Jan;148(1):79-84. doi: 10.1001/archdermatol.2011.262. Epub 2011 Sep 19. Arch Dermatol. 2012. PMID: 21931011 Free PMC article.
-
Treatment options for DOCK8 deficiency-related severe dermatitis.J Dermatol. 2021 Sep;48(9):1386-1393. doi: 10.1111/1346-8138.15955. Epub 2021 May 27. J Dermatol. 2021. PMID: 34043252
-
Clinical, immunological and molecular profiles of DOCK8 deficiency in six patients from a tertiary care centre in North India.Clin Exp Dermatol. 2024 Feb 14;49(3):226-234. doi: 10.1093/ced/llad345. Clin Exp Dermatol. 2024. PMID: 37815217
-
Genetic, clinical, and laboratory markers for DOCK8 immunodeficiency syndrome.Dis Markers. 2010;29(3-4):131-9. doi: 10.3233/DMA-2010-0737. Dis Markers. 2010. PMID: 21178272 Free PMC article. Review.
-
Dedicator of cytokinesis 8 (DOCK8) deficiency.Curr Opin Allergy Clin Immunol. 2010 Dec;10(6):515-20. doi: 10.1097/ACI.0b013e32833fd718. Curr Opin Allergy Clin Immunol. 2010. PMID: 20864884 Free PMC article. Review.
Cited by
-
Autosomal recessive hyper-IgE syndrome caused by DOCK8 gene mutation with new clinical features: a case report.BMC Neurol. 2021 Jul 23;21(1):288. doi: 10.1186/s12883-021-02324-3. BMC Neurol. 2021. PMID: 34301197 Free PMC article.
-
New Insights and Advances in Pathogenesis and Treatment of Very Early Onset Inflammatory Bowel Disease.Front Pediatr. 2022 Mar 1;10:714054. doi: 10.3389/fped.2022.714054. eCollection 2022. Front Pediatr. 2022. PMID: 35299671 Free PMC article. Review.
-
Efficacy of Dupilumab in Treating Atopic Dermatitis With Recurrent Eczema Herpeticum in a Patient With DOCK8-Deficiency Hyper-IgE Syndrome: A Case Report.Cureus. 2023 Aug 12;15(8):e43360. doi: 10.7759/cureus.43360. eCollection 2023 Aug. Cureus. 2023. PMID: 37701007 Free PMC article.
-
Actin cytoskeletal defects in immunodeficiency.Immunol Rev. 2013 Nov;256(1):282-99. doi: 10.1111/imr.12114. Immunol Rev. 2013. PMID: 24117828 Free PMC article. Review.
-
Dedicator of cytokinesis 8-deficient patients have a breakdown in peripheral B-cell tolerance and defective regulatory T cells.J Allergy Clin Immunol. 2014 Dec;134(6):1365-1374. doi: 10.1016/j.jaci.2014.07.042. Epub 2014 Sep 11. J Allergy Clin Immunol. 2014. PMID: 25218284 Free PMC article.
References
-
- Engelhardt KR, McGhee S, Winkler S, Sassi A, Woellner C, Lopez-Herrera G, Chen A, Kim HS, Lloret MG, Schulze I, Ehl S, Thiel J, Pfeifer D, Veelken H, Niehues T, Siepermann K, Weinspach S, Reisli I, Keles S, Genel F, Kutuculer N, Camcioglu Y, Somer A, Karakoc-Aydiner E, Barlan I, Gennery A, Metin A, Degerliyurt A, Pietrogrande MC, Yeganeh M, Baz Z, Al-Tamemi S, Klein C, Puck JM, Holland SM, McCabe ER, Grimbacher B, Chatila TA. Large deletions and point mutations involving the dedicator of cytokinesis 8 (DOCK8) in the autosomal-recessive form of hyper-IgE syndrome. J Allergy Clin Immunol. 2009;124:1289–1302.e1284. - PMC - PubMed
-
- Su HC, Jing H, Zhang Q. DOCK8 deficiency. Ann N Y Acad Sci. 2011;1246:26–33. - PubMed
-
- Renner ED, Puck JM, Holland SM, Schmitt M, Weiss M, Frosch M, Bergmann M, Davis J, Belohradsky BH, Grimbacher B. Autosomal recessive hyperimmunoglobulin E syndrome: a distinct disease entity. J Pediatr. 2004;144:93–99. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
