

Atherosclerosis, inflammation, genetics, and stem cells: 2012 update
- PMID: 22476914
- PMCID: PMC3537163
- DOI: 10.1007/s11883-012-0244-1
Atherosclerosis, inflammation, genetics, and stem cells: 2012 update
Abstract
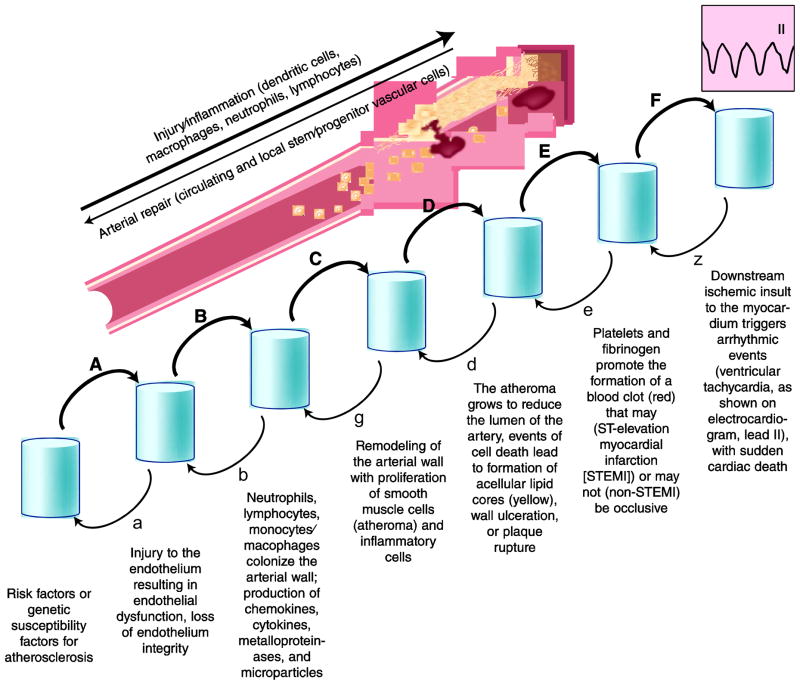
Atherosclerosis is a peculiar form of inflammation triggered by cholesterol-rich lipoproteins and other noxious factors such as cigarette smoke, diabetes mellitus, and hypertension. Genetics also play an important role in the disease, accounting for about 40% of the risk. Of surprise in recent years of post-human genome sequencing, atherosclerosis-relevant genes discovered by non-biased techniques (ie, genome-wide association studies), did not rehash previously suspected pathways of lipid metabolism, diabetes, or hypertension. Instead these studies highlighted genes relevant to mechanisms of inflammation and stem cell biology. Only a minority of implicated genes were linked to lipid and other cardiac risk factor genes. Although such findings do not contradict the fact that atherosclerosis is triggered and exacerbated by elevated lipids, atherosclerosis "new genes" suggest that the mechanism responsible for the development of arterial lesions is more complex than a simple response to injury, where injury is necessary, but perhaps not sufficient, for disease progression.
Figures
References
-
- Brown MS, Goldstein JL. Koch's postulates for cholesterol. Cell. 1992;71(2):187–188. - PubMed
-
- Libby P, Ridker PM, Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature. 2011;473(7347):317–25. Review. • This is a thorough review of the most recent information on atherosclerosis inflammation and its cellular and molecular agents. Novel clinical trials with anti-inflammatory drugs are also surveyed. - PubMed
-
- Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med. 2002;347(20):1557–1565. - PubMed
-
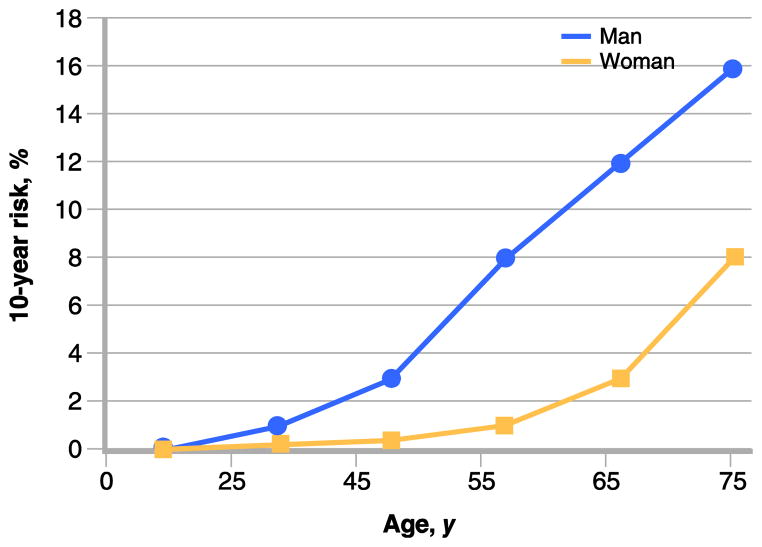
- American Heart Association. [Accessed December 2011.];Heart Attack Risk Calculator. Available at: https://www.heart.org/gglRisk/locale/en_US/index.html?gtype=health.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
