

Effects of age and weight-based dosing of enoxaparin on anti-factor xa levels in pediatric patients
- PMID: 22477802
- PMCID: PMC3018183
Effects of age and weight-based dosing of enoxaparin on anti-factor xa levels in pediatric patients
Abstract
Objective: The objective of this dose range study is to expand on the relationship between age and weight-based doses of enoxaparin and resulting levels of anti-factor Xa (anti-Xa) in pediatric patients. The primary outcome of this study is to determine the average dose of enoxaparin required to produce a therapeutic effect. Secondary outcomes include the number of enoxaparin dose changes required to achieve a therapeutic level of anti-Xa in each age group, the success rates of achieving and maintaining therapeutic anti-Xa levels, and the effect of serum antithrombin concentrations on anti-Xa levels. The study will also determine whether different dispensed concentrations of enoxaparin play a role in achieving therapeutic levels of anti-Xa.
Methods: Single center, retrospective chart review. Patients were excluded from the study if they were older than 18 years of age, were receiving enoxaparin for prophylactic purposes, had a creatinine clearance < 30 ml/min/1.73m(2), and if no anti-factor Xa levels were drawn.
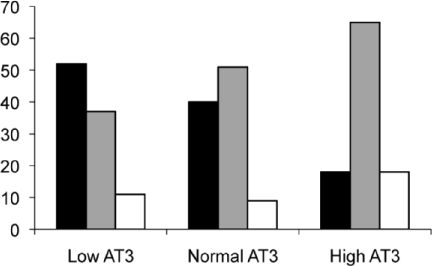
Results: Average enoxaparin doses required for therapeutic levels of anti-factor Xa were 1.8 mg/kg for patients <1 month, 1.64 mg/kg (1 month to 1 year), 1.45 mg/kg (1 to 6 years), and 1.05 mg/kg (>6 years of age). An average of 3.24 dose changes was required for neonates to achieve therapeutic levels anti-factor Xa. The success rates for achieving and maintaining therapeutic levels were both 41%. Patients with low serum antithrombin levels were more likely to have low anti-Xa levels than those with normal or high values, 52% vs 40% vs 18%, respectively. Patients receiving diluted concentrations, 10 or 20 mg/mL, experienced lower anti-Xa levels than patients who received the standard manufactured concentration of 100 mg/mL, 61% vs 33%.
Conclusion: Based on this dose-range study, enoxaparin should be initiated at larger doses than recommended by the current guidelines to promptly achieve therapeutic anti-Xa levels. Doses should be divided into three age groups instead of two as currently suggested in the guidelines. To increase the likelihood of achieving therapeutic levels, the commercially available enoxaparin product should not be diluted if possible.
Figures
References
-
- Punzalan RC, Hillery CA, Montgomery RR, et al. Low molecular weight heparin in thrombotic disease in children and adolescents. J Pediatr Hematol Oncol. 2000;22:137–142. - PubMed
-
- Hyers TM, Agnelli G, Hull RD, et al. Antithrombotic therapy for thromboembolic disease. Chest. 2001;119:176S–193S. - PubMed
-
- Fareed J, Hoppensteadt D, Walenga J, et al. Pharmacodynamic and pharmacokinetic properties of enoxaparin: implications for clinical practice. Clin Pharmacokinet. 2003;42:1043–57. - PubMed
-
- Malowany JI, Knoppert DC, Chan AKC, et al. Enoxaparin use in the neonatal intensive care unit: experience over 8 years. Pharmacotherapy. 2007;27:1263–1271. - PubMed
-
- Monagle P, Michelson AD, Bovill E, et al. Antithrombotic therapy in children. Chest. 2001;119:344–370. - PubMed
LinkOut - more resources
Full Text Sources