

Impact of multi-targeted antiretroviral treatment on gut T cell depletion and HIV reservoir seeding during acute HIV infection
- PMID: 22479485
- PMCID: PMC3316511
- DOI: 10.1371/journal.pone.0033948
Impact of multi-targeted antiretroviral treatment on gut T cell depletion and HIV reservoir seeding during acute HIV infection
Abstract
Background: Limited knowledge exists on early HIV events that may inform preventive and therapeutic strategies. This study aims to characterize the earliest immunologic and virologic HIV events following infection and investigates the usage of a novel therapeutic strategy.
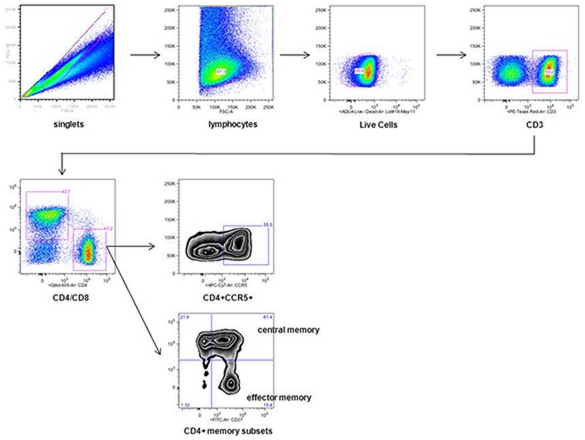
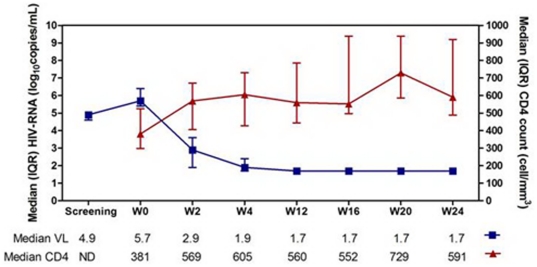
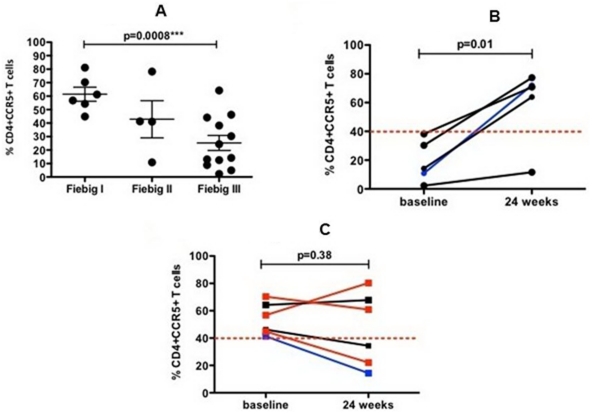
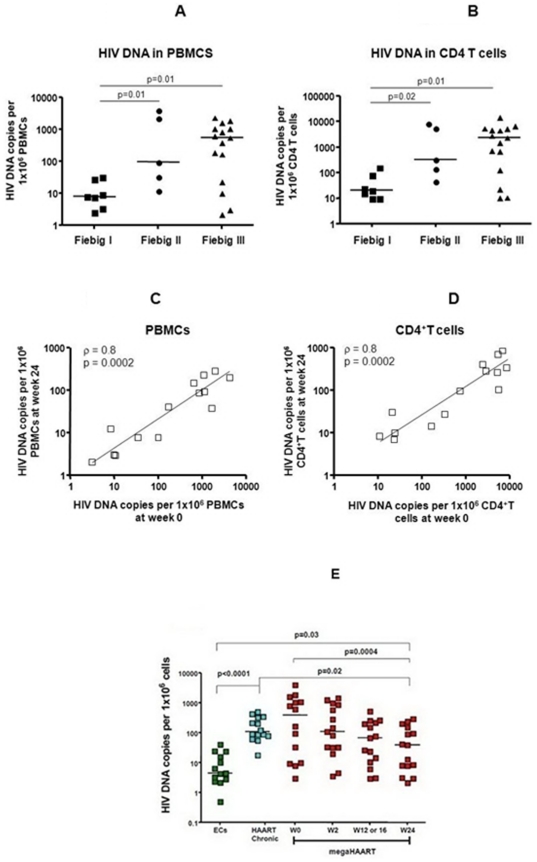
Methods and findings: We prospectively screened 24,430 subjects in Bangkok and identified 40 AHI individuals. Thirty Thais were enrolled (8 Fiebig I, 5 Fiebig II, 15 Fiebig III, 2 Fiebig IV) of whom 15 completed 24 weeks of megaHAART (tenofovir/emtricitabine/efavirenz/raltegravir/maraviroc). Sigmoid biopsies were completed in 24/30 at baseline and 13/15 at week 24. At baseline, the median age was 29 years and 83% were MSM. Most were symptomatic (87%), and were infected with R5-tropic (77%) CRF01_AE (70%). Median CD4 was 406 cells/mm(3). HIV RNA was 5.5 log(10) copies/ml. Median total blood HIV DNA was higher in Fiebig III (550 copy/10(6) PBMC) vs. Fiebig I (8 copy/10(6) PBMC) (p = 0.01) while the median %CD4+CCR5+ gut T cells was lower in Fiebig III (19%) vs. Fiebig I (59%) (p = 0.0008). After 24 weeks of megaHAART, HIV RNA levels of <50 copies were achieved in 14/15 in blood and 13/13 in gut. Total blood HIV DNA at week 0 predicted reservoir size at week 24 (p<0.001). Total HIV DNA declined significantly and was undetectable in 3 of 15 in blood and 3 of 7 in gut. Frequency of CD4+CCR5+ gut T cells increased from 41% at baseline to 64% at week 24 (p>0.050); subjects with less than 40% at baseline had a significant increase in CD4+CCR5+ T cells from baseline to week 24 (14% vs. 71%, p = 0.02).
Conclusions: Gut T cell depletion and HIV reservoir seeding increases with progression of AHI. MegaHAART was associated with immune restoration and reduced reservoir size. Our findings could inform research on strategies to achieve HIV drug-free remission.
Conflict of interest statement
Figures


References
-
- Hutter G, Nowak D, Mossner M, Ganepola S, Mussig A, et al. Long-term control of HIV by CCR5 Delta32/Delta32 stem-cell transplantation. N Engl J Med. 2009;360:692–698. - PubMed
-
- Trono D, Van Lint C, Rouzioux C, Verdin E, Barre-Sinoussi F, et al. HIV persistence and the prospect of long-term drug-free remissions for HIV-infected individuals. Science. 2010;329:174–180. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
