

High-frequency oscillations (HFOs) in clinical epilepsy
- PMID: 22480752
- PMCID: PMC3674884
- DOI: 10.1016/j.pneurobio.2012.03.001
High-frequency oscillations (HFOs) in clinical epilepsy
Abstract
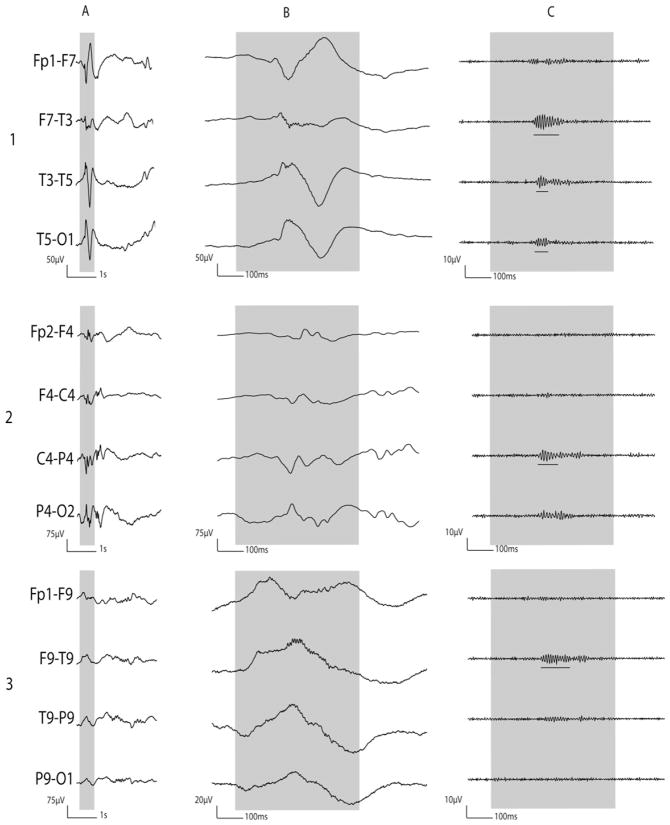
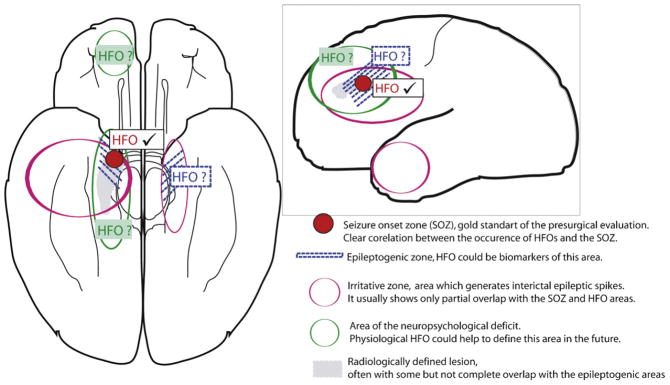
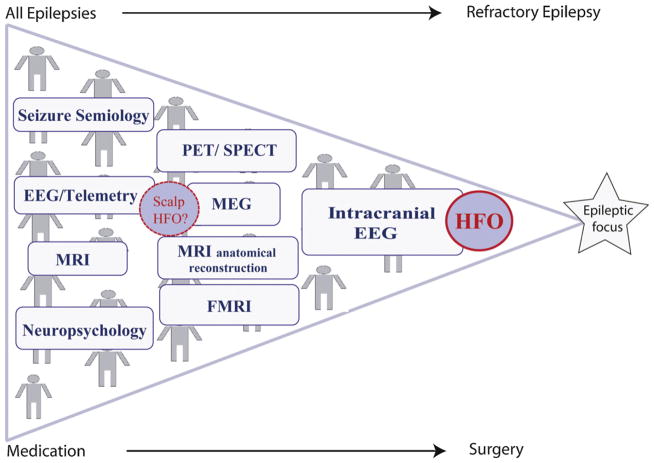
Epilepsy is one of the most frequent neurological diseases. In focal medically refractory epilepsies, successful surgical treatment largely depends on the identification of epileptogenic zone. High-frequency oscillations (HFOs) between 80 and 500Hz, which can be recorded with EEG, may be novel markers of the epileptogenic zone. This review discusses the clinical importance of HFOs as markers of epileptogenicity and their application in different types of epilepsies. HFOs are clearly linked to the seizure onset zone, and the surgical removal of regions generating them correlates with a seizure free post-surgical outcome. Moreover, HFOs reflect the seizure-generating capability of the underlying tissue, since they are more frequent after the reduction of antiepileptic drugs. They can be successfully used in pediatric epilepsies such as epileptic spasms and help to understand the generation of this specific type of seizures. While mostly recorded on intracranial EEGs, new studies suggest that identification of HFOs on scalp EEG or magnetoencephalography (MEG) is possible as well. Thus not only patients with refractory epilepsies and invasive recordings but all patients might profit from the analysis of HFOs. Despite these promising results, the analysis of HFOs is not a routine clinical procedure; most results are derived from relatively small cohorts of patients and many aspects are not yet fully understood. Thus the review concludes that even if HFOs are promising biomarkers of epileptic tissue, there are still uncertainties about mechanisms of generation, methods of analysis, and clinical applicability. Large multicenter prospective studies are needed prior to widespread clinical application.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
References
-
- Agirre-Arrizubieta Z, Huiskamp GJ, Ferrier CH, van Huffelen AC, Leijten FS. Interictal magnetoencephalography and the irritative zone in the electrocorticogram. Brain. 2009;132:3060–3071. - PubMed
-
- Allen PJ, Fish DR, Smith SJ. Very high-frequency rhythmic activity during SEEG suppression in frontal lobe epilepsy. Electroencephalography and Clinical Neurophysiology. 1992;82:155–159. - PubMed
-
- Aubert S, Wendling F, Regis J, McGonigal A, Figarella-Branger D, Peragut JC. Local and remote epileptogenicity in focal cortical dysplasias and neurodevelopmental tumours. Brain. 2009;132:3072–3086. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
