

Quantification and impact of untreated coronary artery disease after percutaneous coronary intervention: the residual SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) score
- PMID: 22483327
- PMCID: PMC3725642
- DOI: 10.1016/j.jacc.2012.03.010
Quantification and impact of untreated coronary artery disease after percutaneous coronary intervention: the residual SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) score
Abstract
Objectives: The purpose of this study was to quantify the extent and complexity of residual coronary stenoses following percutaneous coronary intervention (PCI) and to evaluate its impact on adverse ischemic outcomes.
Background: Incomplete revascularization (IR) after PCI is common, and most studies have suggested that IR is associated with a worse prognosis compared with complete revascularization (CR). However, formal quantification of the extent and complexity of residual atherosclerosis after PCI has not been performed.
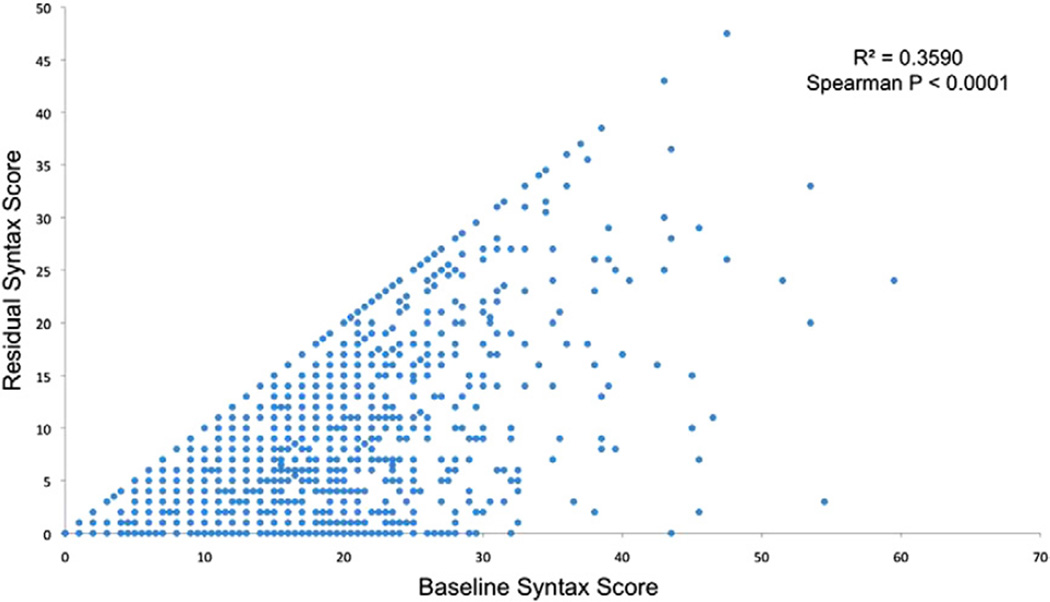
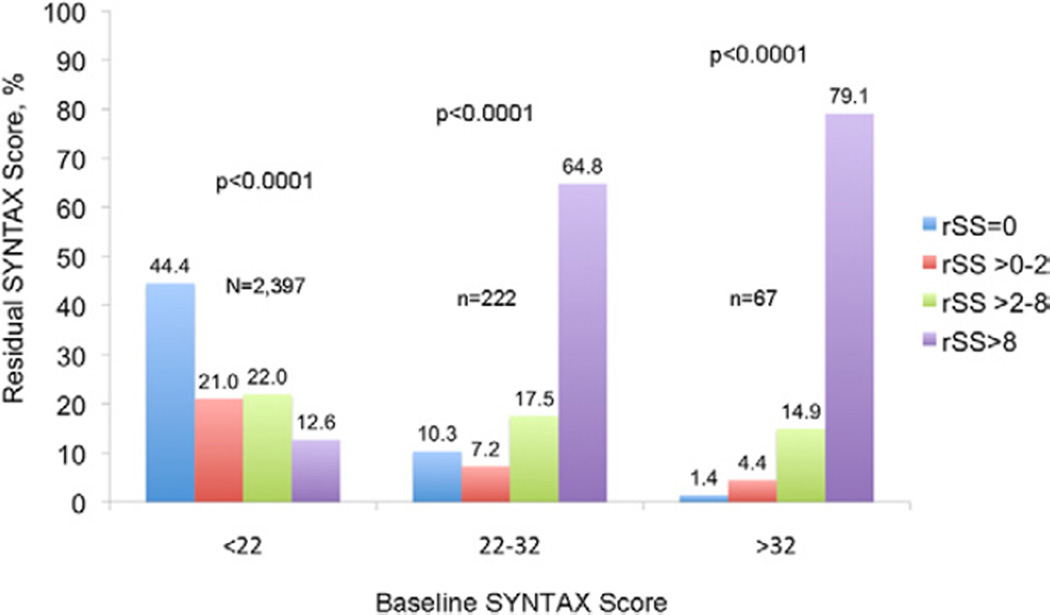
Methods: The baseline Synergy Between PCI With Taxus and Cardiac Surgery (SYNTAX) score (bSS) from 2,686 angiograms from patients with moderate- and high-risk acute coronary syndrome (ACS) undergoing PCI enrolled in the prospective ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trial was determined. The SS after PCI was also assessed, generating the "residual" SS (rSS). Patients with rSS >0 were defined as having IR and were stratified by rSS tertiles, and their outcomes were compared to the CR group.
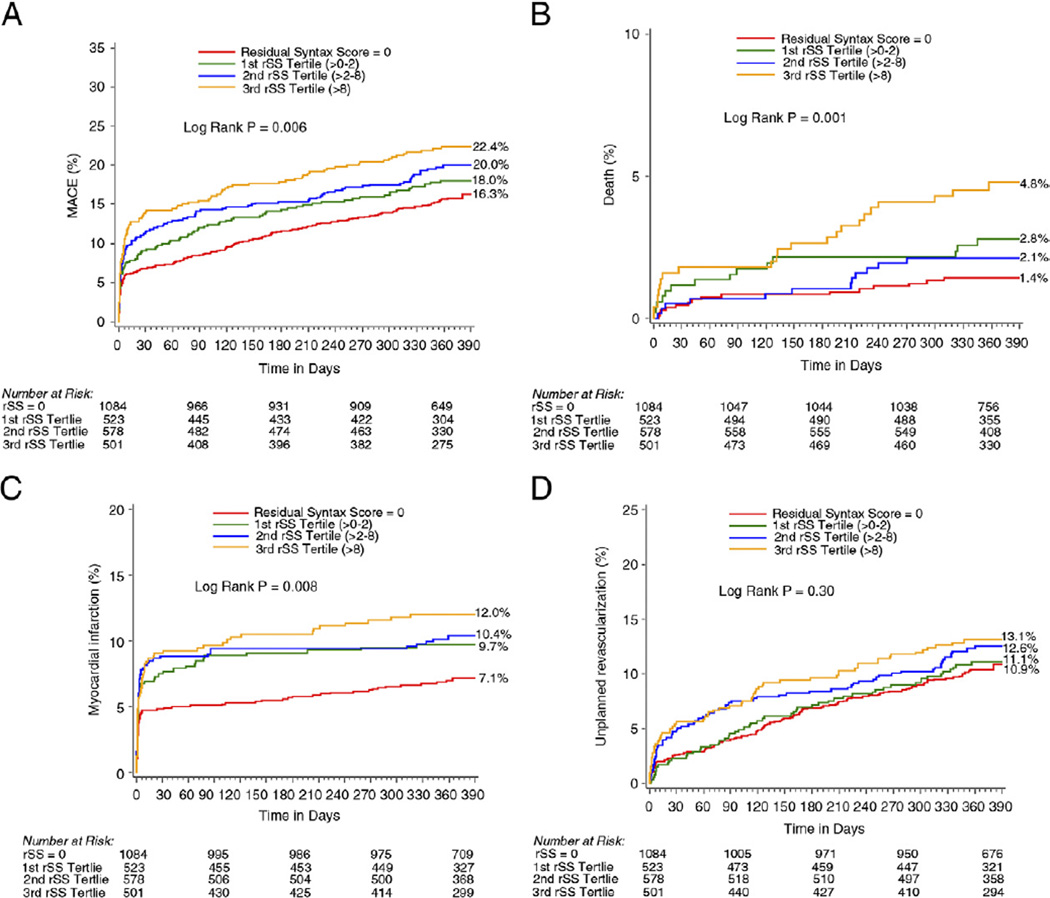
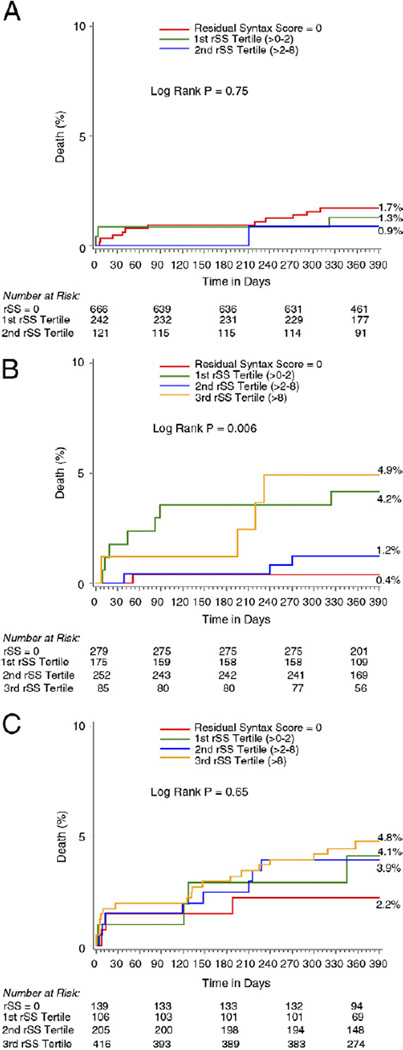
Results: The bSS was 12.8 ± 6.7, and after PCI the rSS was 5.6 ± 2.2. Following PCI, 1,084 patients (40.4%) had rSS = 0 (CR), 523 (19.5%) had rSS >0 but ≤2, 578 (21.5%) had rSS >2 but ≤8, and 501 patients (18.7%) had rSS >8. Age, insulin-treated diabetes, hypertension, smoking, elevated biomarkers or ST-segment deviation, and lower ejection fraction were more frequent in patients with IR compared with CR. The 30-day and 1-year rates of ischemic events were significantly higher in the IR group compared with the CR group, especially those with high rSS. By multivariable analysis, rSS was a strong independent predictor of all ischemic outcomes at 1 year, including all-cause mortality (hazard ratio: 1.05, 95% confidence interval: 1.02 to 1.09, p = 0.006).
Conclusions: The rSS is useful to quantify and risk-stratify the degree and complexity of residual stenosis after PCI. Specifically, rSS >8.0 after PCI in patients with moderate- and high-risk ACS is associated with a poor 30-day and 1-year prognosis. (Comparison of Angiomax Versus Heparin in Acute Coronary Syndromes; NCT00093158).
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Left main or multivessel coronary revascularization: applying both anatomy and physiology to individualize care.Future Cardiol. 2017 Jul;13(4):317-322. doi: 10.2217/fca-2017-0026. Epub 2017 Jun 23. Future Cardiol. 2017. PMID: 28644053 No abstract available.
References
-
- Rogers WJ, Bourassa MG, Andrews TC, et al. Asymptomatic Cardiac Ischemia Pilot (ACIP) study: outcome at 1 year for patients with asymptomatic cardiac ischemia randomized to medical therapy or revascularization. The ACIP investigators. J Am Coll Cardiol. 1995;26:594–605. - PubMed
-
- Hannan EL, Racz M, Holmes DR, et al. Impact of completeness of percutaneous coronary intervention revascularization on long-term outcomes in the stent era. Circulation. 2006;113:2406–2412. - PubMed
-
- Hannan EL, Wu C, Walford G, et al. Incomplete revascularization in the era of drug-eluting stents: impact on adverse outcomes. J Am Coll Cardiol Intv. 2009;2:17–25. - PubMed
-
- Kim YH, Park DW, Lee JY, et al. Impact of angiographic complete revascularization after drug-eluting stent implantation or coronary artery bypass graft surgery for multivessel coronary artery disease. Circulation. 2011;123:2373–2381. - PubMed
-
- van den Brand MJ, Rensing BJ, Morel MA, et al. The effect of completeness of revascularization on event-free survival at one year in the ARTS trial. J Am Coll Cardiol. 2002;39:559–564. - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
