

Normalization of tumour blood vessels improves the delivery of nanomedicines in a size-dependent manner
- PMID: 22484912
- PMCID: PMC3370066
- DOI: 10.1038/nnano.2012.45
Normalization of tumour blood vessels improves the delivery of nanomedicines in a size-dependent manner
Abstract
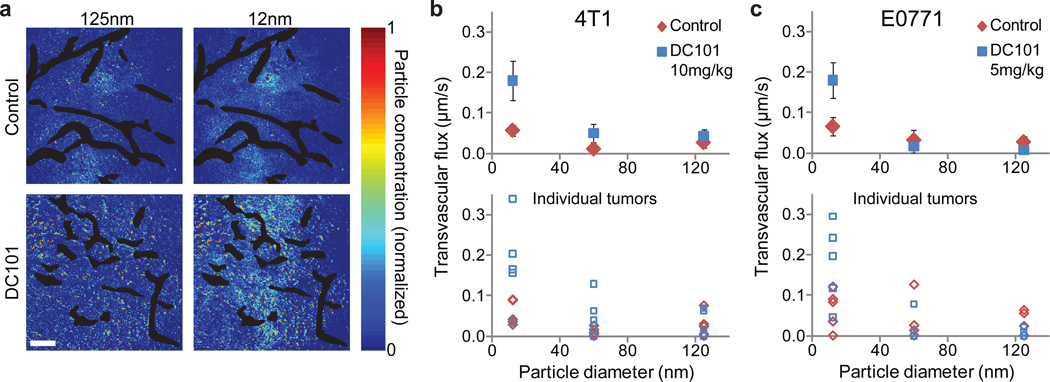
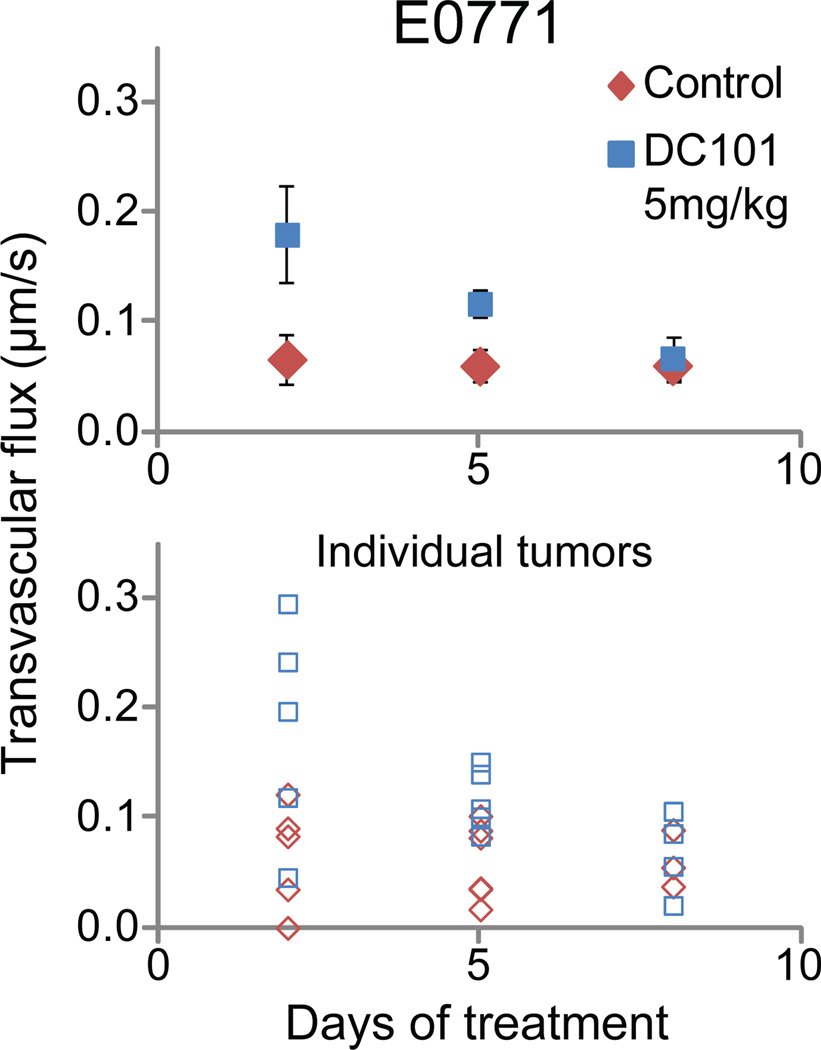
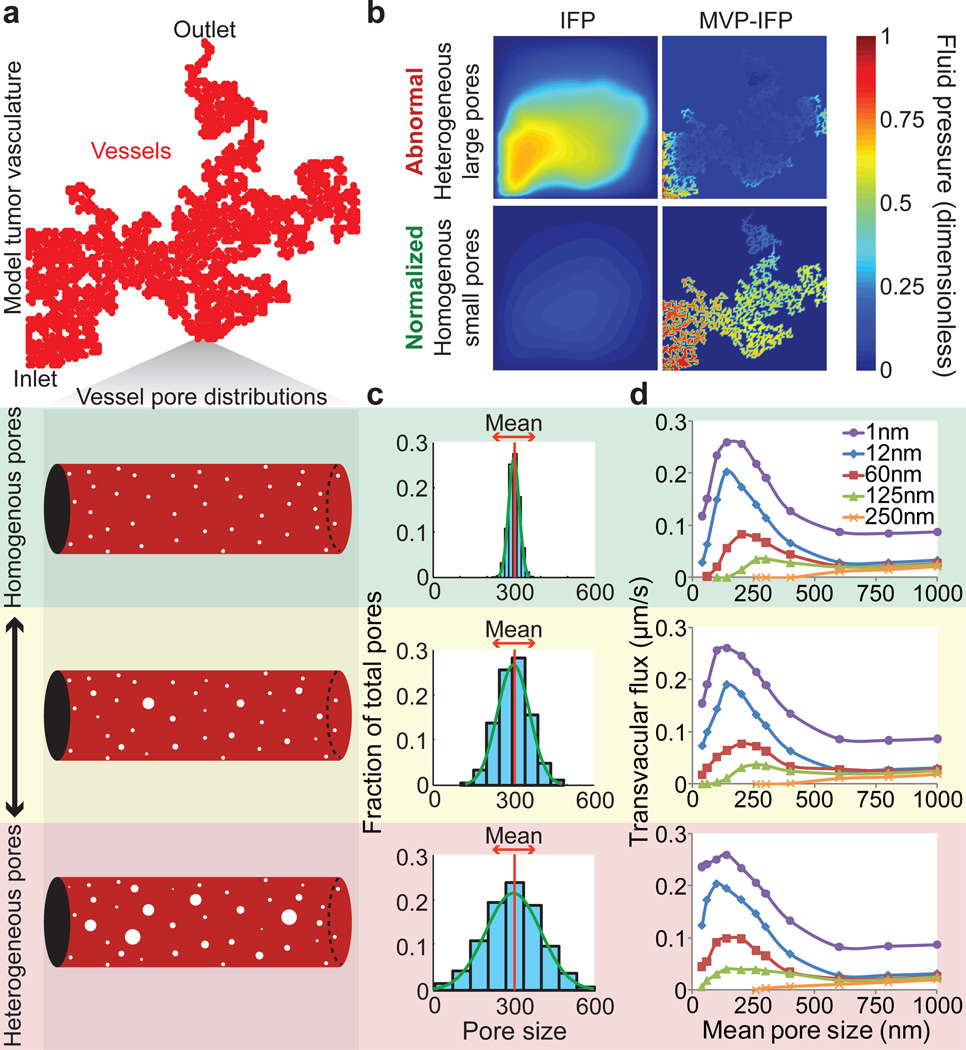
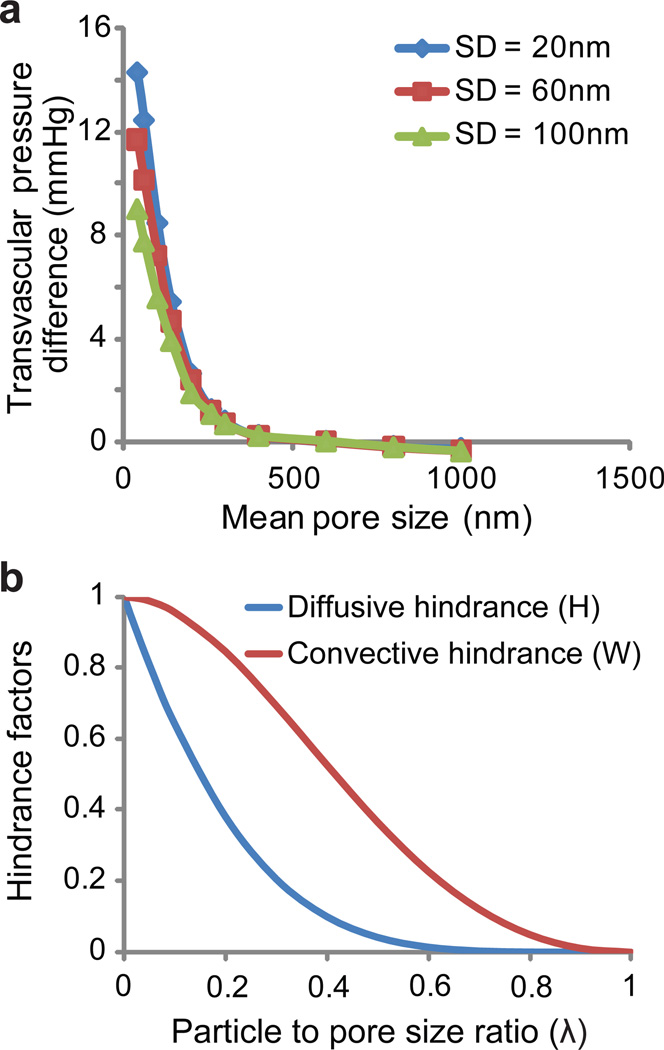
The blood vessels of cancerous tumours are leaky and poorly organized. This can increase the interstitial fluid pressure inside tumours and reduce blood supply to them, which impairs drug delivery. Anti-angiogenic therapies--which 'normalize' the abnormal blood vessels in tumours by making them less leaky--have been shown to improve the delivery and effectiveness of chemotherapeutics with low molecular weights, but it remains unclear whether normalizing tumour vessels can improve the delivery of nanomedicines. Here, we show that repairing the abnormal vessels in mammary tumours, by blocking vascular endothelial growth factor receptor-2, improves the delivery of smaller nanoparticles (diameter, 12 nm) while hindering the delivery of larger nanoparticles (diameter, 125 nm). Using a mathematical model, we show that reducing the sizes of pores in the walls of vessels through normalization decreases the interstitial fluid pressure in tumours, thus allowing small nanoparticles to enter them more rapidly. However, increased steric and hydrodynamic hindrances, also associated with smaller pores, make it more difficult for large nanoparticles to enter tumours. Our results further suggest that smaller (∼12 nm) nanomedicines are ideal for cancer therapy due to their superior tumour penetration.
Figures
Comment in
-
Nanomedicine: Downsizing tumour therapeutics.Nat Nanotechnol. 2012 Jun 6;7(6):346-7. doi: 10.1038/nnano.2012.89. Nat Nanotechnol. 2012. PMID: 22669087 Free PMC article. No abstract available.
-
Improving nanoparticle delivery with anti-angiogenesis therapy.Nanomedicine (Lond). 2012 Jul;7(7):949-50. doi: 10.2217/nnm.12.68. Nanomedicine (Lond). 2012. PMID: 22846089 No abstract available.
-
The importance of size: nanomedicine for delivery of anticancer drugs in solid tumors.Nanomedicine (Lond). 2012 Sep;7(9):1294-5. Nanomedicine (Lond). 2012. PMID: 23162864 No abstract available.
References
-
- Nagy JA, Dvorak AM, Dvorak HF. VEGF-A and the induction of pathological angiogenesis. Annu. Rev. Pathol. 2007;2:251–275. - PubMed
-
- Yuan F, et al. Microvascular permeability and interstitial penetration of sterically stabilized (stealth) liposomes in a human tumor xenograft. Cancer Res. 1994;54:3352–3356. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- T32 CA073479/CA/NCI NIH HHS/United States
- R01 CA126642/CA/NCI NIH HHS/United States
- R01-CA085140/CA/NCI NIH HHS/United States
- R01-CA098706/CA/NCI NIH HHS/United States
- R01 CA098706/CA/NCI NIH HHS/United States
- R01 CA085140/CA/NCI NIH HHS/United States
- R01-CA115767/CA/NCI NIH HHS/United States
- P01-CA080124/CA/NCI NIH HHS/United States
- R24 CA085140/CA/NCI NIH HHS/United States
- R01-CA096915/CA/NCI NIH HHS/United States
- R01 CA115767/CA/NCI NIH HHS/United States
- P01 CA080124/CA/NCI NIH HHS/United States
- R01-CA126642/CA/NCI NIH HHS/United States
- R01 CA096915/CA/NCI NIH HHS/United States
- T32-CA073479/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
