

Measuring adiposity in patients: the utility of body mass index (BMI), percent body fat, and leptin
- PMID: 22485140
- PMCID: PMC3317663
- DOI: 10.1371/journal.pone.0033308
Measuring adiposity in patients: the utility of body mass index (BMI), percent body fat, and leptin
Abstract
Background: Obesity is a serious disease that is associated with an increased risk of diabetes, hypertension, heart disease, stroke, and cancer, among other diseases. The United States Centers for Disease Control and Prevention (CDC) estimates a 20% obesity rate in the 50 states, with 12 states having rates of over 30%. Currently, the body mass index (BMI) is most commonly used to determine adiposity. However, BMI presents as an inaccurate obesity classification method that underestimates the epidemic and contributes to failed treatment. In this study, we examine the effectiveness of precise biomarkers and duel-energy x-ray absorptiometry (DXA) to help diagnose and treat obesity.
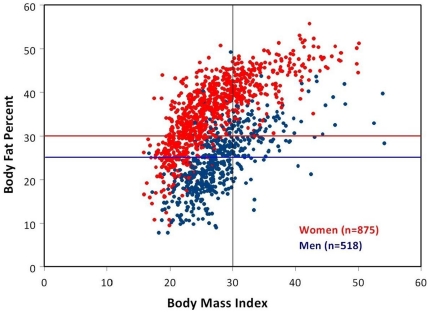
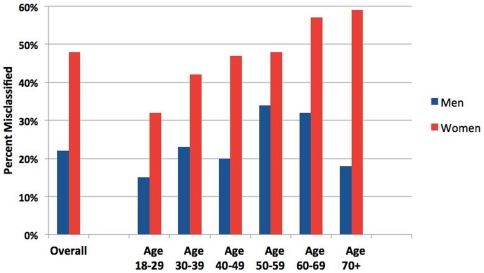
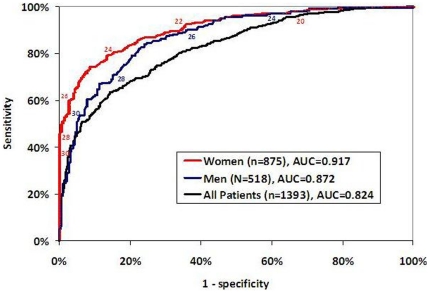
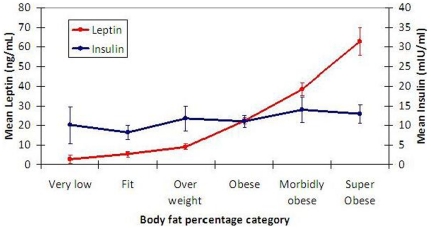
Methodology/principal findings: A cross-sectional study of adults with BMI, DXA, fasting leptin and insulin results were measured from 1998-2009. Of the participants, 63% were females, 37% were males, 75% white, with a mean age = 51.4 (SD = 14.2). Mean BMI was 27.3 (SD = 5.9) and mean percent body fat was 31.3% (SD = 9.3). BMI characterized 26% of the subjects as obese, while DXA indicated that 64% of them were obese. 39% of the subjects were classified as non-obese by BMI, but were found to be obese by DXA. BMI misclassified 25% men and 48% women. Meanwhile, a strong relationship was demonstrated between increased leptin and increased body fat.
Conclusions/significance: Our results demonstrate the prevalence of false-negative BMIs, increased misclassifications in women of advancing age, and the reliability of gender-specific revised BMI cutoffs. BMI underestimates obesity prevalence, especially in women with high leptin levels (>30 ng/mL). Clinicians can use leptin-revised levels to enhance the accuracy of BMI estimates of percentage body fat when DXA is unavailable.
Conflict of interest statement
Figures
References
-
- Jia H, Lubetkin EI. Trends in quality-adjusted life-years lost contributed by smoking and obesity. Am J Prev Med. 2010;38(2):138–44. - PubMed
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: Systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet. 2011;378(9785):31–40. - PubMed
-
- Malnick SD, Knobler H. The medical complications of obesity. QJM. 2006;99(9):565–79. - PubMed
-
- Gallagher D, Visser M, Sepulveda D, Pierson RN, Harris T, et al. How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups? Am J Epidemiol. 1996;143(3):228–39. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
