

Inverted papillomas and benign nonneoplastic lesions of the nasal cavity
- PMID: 22487294
- PMCID: PMC3906506
- DOI: 10.2500/ajra.2012.26.3732
Inverted papillomas and benign nonneoplastic lesions of the nasal cavity
Abstract
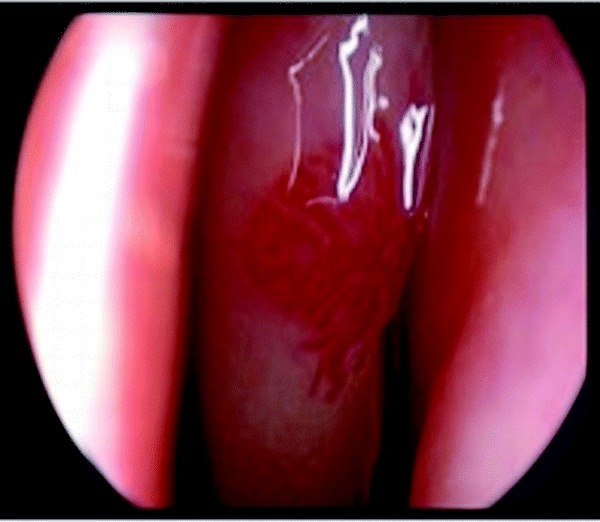
Background: Benign lesions of the nasal cavity represent a diverse group of pathologies. Furthermore, each of these disorders may present differently in any given patient as pain and discomfort, epistaxis, headaches, vision changes, or nasal obstruction. Although these nasal masses are benign, many of them have a significant capacity for local tissue destruction and symptomatology secondary to this destruction. Advances in office-based endoscopic nasendoscopy have equipped the otolaryngologist with a safe, inexpensive, and rapid means of directly visualizing lesions within the nasal cavity and the initiation of appropriate treatment.
Methods: The purpose of this study is to review the diagnosis, management, and controversies of many of the most common benign lesions of the nasal cavity encountered by the primary care physician or otolaryngologist.
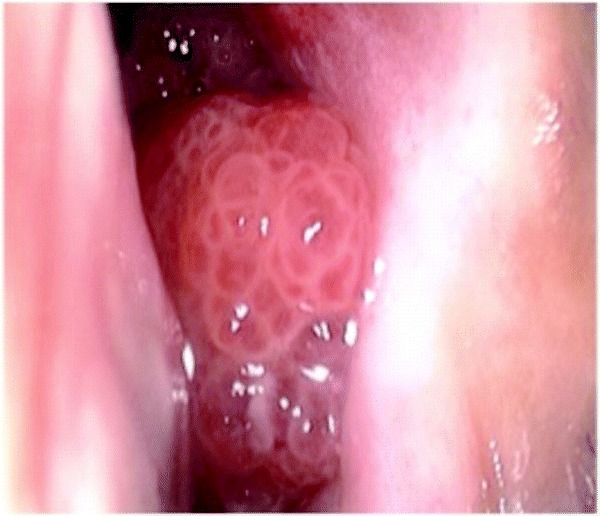
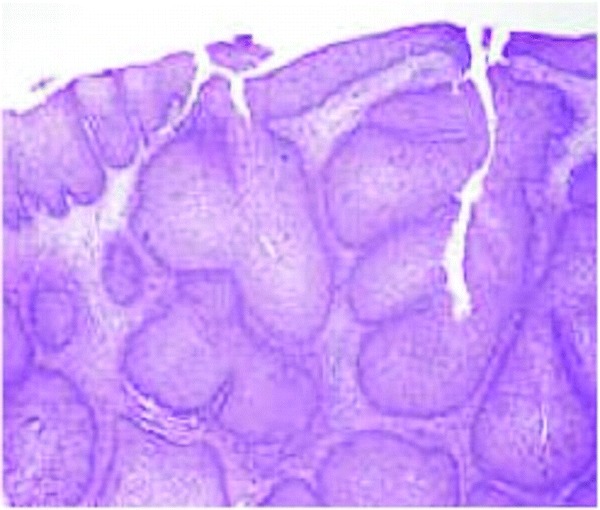
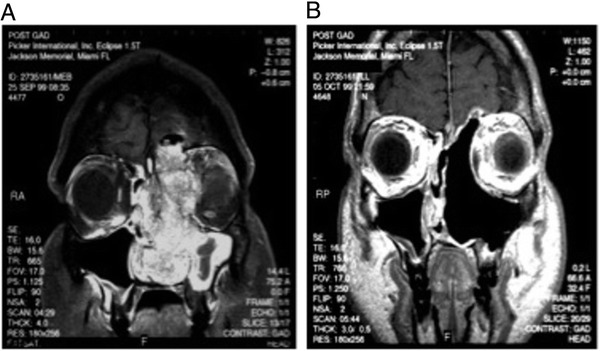
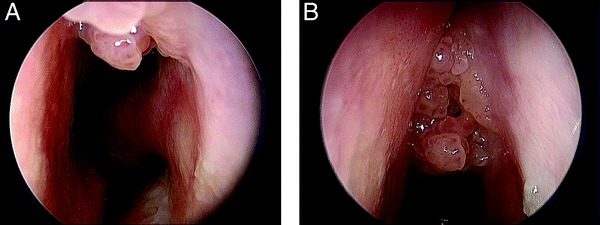
Results: This includes discussion of inverted papilloma (IP), juvenile angiofibroma, squamous papilloma, pyogenic granuloma, hereditary hemorrhagic telangiectasia, schwannoma, benign fibro-osseous lesions, and other benign lesions of the nasal cavity, with particular emphasis on IP and juvenile angiofibroma.
Conclusion: A diverse array of benign lesions occur within the nasal cavity and paranasal cavities. Despite their inability to metastasize, many of these lesions have significant capability for local tissue destruction and recurrence.
Conflict of interest statement
The authors have no conflicts of interest to declare pertaining to this article
Figures
References
-
- Cody DT, II, DeSanto LW. Neoplasm of the nasal cavity. In Otolaryngology Head and Neck Surgery, Vol. 2, ed. 3 Cumming CW FJ, Harker LA, Krause CJ, et al. (Eds). St. Louis, MO: Mosby-Year Book, Inc., 883–901, 1998.
-
- Caruana SM, Zwiebel N, Cocker R, McCormick SA, et al. p53 Alteration and human papilloma virus in paranasal sinus cancer. Cancer 79:1320–1328, 1997. - PubMed
-
- Ringert N. Pathology of malignant tumors arising in the nasal and paranasal cavities and maxilla. Acta Otolaryngol (Stockh) 27(suppl):31–42, 1938.
-
- Furata YST, Nagashima K, Inoue K, et al. Molecular pathological study of human papillomavirus infection in inverted papilloma and squamous cell carcinoma of the nasal cavities and paranasal sinuses. Laryngoscope 101:79–85, 1991. - PubMed
-
- Herrold KM. Epithelial papillomas of the nasal cavity. Arch Pathol 78:189–195, 1964. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
