

Prevalent pregnancy, biological sex, and virologic response to antiretroviral therapy
- PMID: 22487586
- PMCID: PMC3404188
- DOI: 10.1097/QAI.0b013e318256b310
Prevalent pregnancy, biological sex, and virologic response to antiretroviral therapy
Abstract
Objective: Pregnancy is a common indication for initiation of highly active antiretroviral therapy (HAART) in sub-Saharan Africa. Our objective was to evaluate how pregnancy at treatment initiation predicts virologic response to HAART.
Methods: We evaluated an open cohort of 9173 patients who initiated HAART between April 2004 and September 2009 in the Themba Lethu Clinic in Johannesburg, South Africa. Risk ratios were estimated using log-binomial regression; hazard ratios were estimated using Cox proportional hazards models; time ratios were estimated using accelerated failure time models. We controlled for calendar date, age, ethnicity, employment status, history of smoking, tuberculosis, WHO stage, weight, body mass index, hemoglobin, CD4 count and CD4 percent, and whether clinical care was free. Extensive sensitivity and secondary analyses were performed.
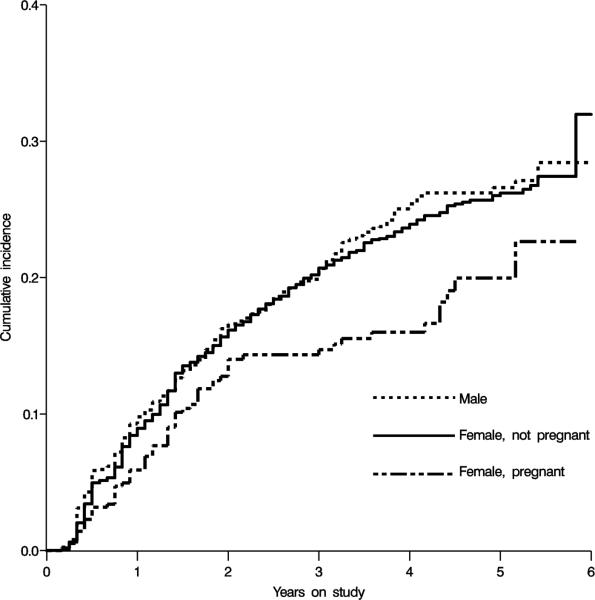
Results: During follow-up, 822 nonpregnant women and 70 pregnant women experienced virologic failure. In adjusted analyses, pregnancy at baseline was associated with reduced risk of virologic failure by 6 months [risk ratio 0.66, 95% confidence limits (CL): 0.35 to 1.22] and with reduced hazard of virologic failure over follow-up (hazard ratio: 0.69, 95% CL: 0.50 to 0.95). The adjusted time ratio for failure was 1.44 (95% CL: 1.13 to 1.84), indicating 44% longer time to event among women pregnant at baseline. Sensitivity analyses generally confirmed main findings.
Conclusions: Pregnancy at HAART initiation is not associated with increased risk of virologic failure at 6 months or during longer follow-up.
Figures
References
-
- UNAIDS [6 July 2010];AIDS Epidemic Update. 2009 http://wwwunaidsorg/en/dataanalysis/epidemiology/2009aidsepidemicupdate/ 2009; Available from.
-
- Pettifor AE, Rees HV, Kleinschmidt I, Steffenson AE, MacPhail C, Hlongwa-Madikizela L, et al. Young people's sexual health in South Africa: HIV prevalence and sexual behaviors from a nationally representative household survey. Aids. 2005;19(14):1525–34. - PubMed
-
- UNAIDS/WHO . AIDS Epidemic Update 2007. Geneva: 2007.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
