

Fibroblast growth factor 23 and adverse clinical outcomes in chronic kidney disease
- PMID: 22487610
- PMCID: PMC3353875
- DOI: 10.1097/MNH.0b013e328351a391
Fibroblast growth factor 23 and adverse clinical outcomes in chronic kidney disease
Abstract
Purpose of review: The aim is to review data on the epidemiology of fibroblast growth factor 23 (FGF23) and adverse clinical outcomes in chronic kidney disease (CKD) and introduce recent insights into the pathophysiology behind the observed relationships.
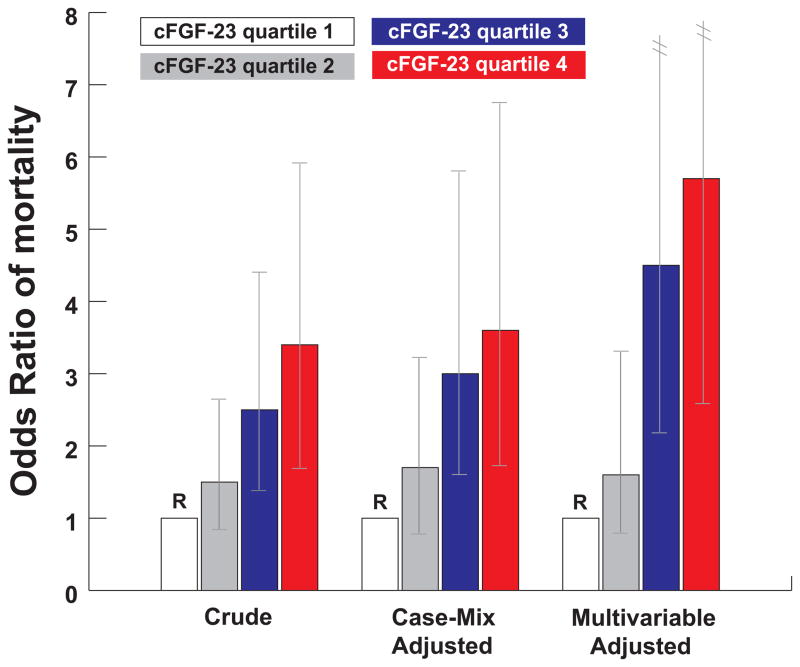
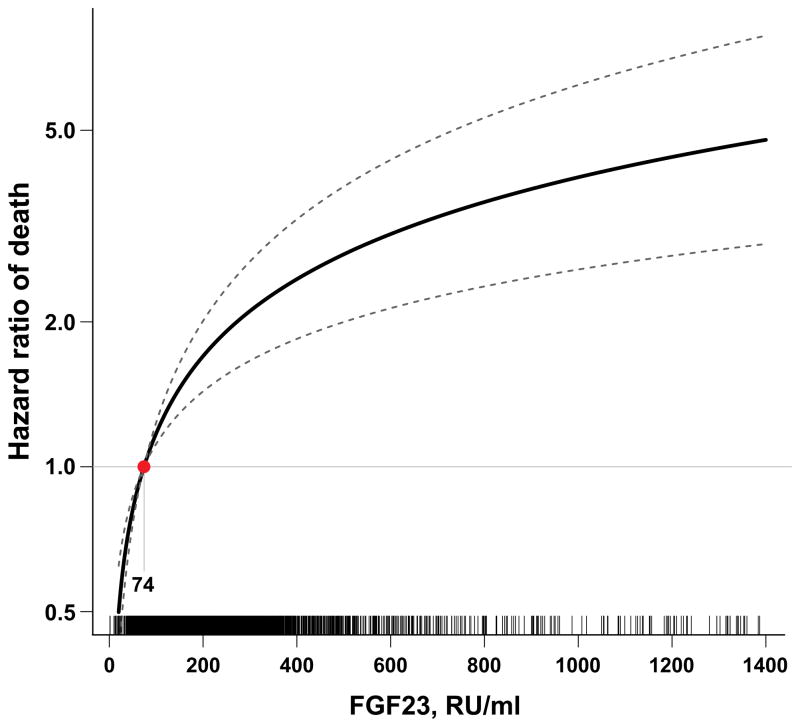
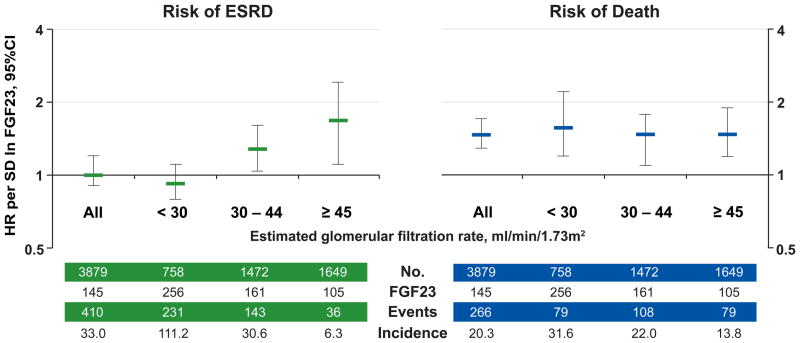
Recent findings: End-stage renal disease and cardiovascular disease are frequent events in patients with CKD, in whom cardiovascular disease is the leading cause of death. Elevated levels of FGF23, a phosphate and vitamin D-regulating hormone, have been associated with risks of end-stage renal disease, cardiovascular disease and mortality. FGF23 excess has also been linked with left-ventricular hypertrophy, and innovative translational experiments have recently established direct end-organ toxicity of FGF23, which induced left-ventricular hypertrophy in animals.
Summary: FGF23 is emerging as a novel risk factor in CKD. Future studies should determine whether interventions that lower FGF23 levels improve clinical outcomes in CKD.
Figures
References
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038–2047. - PubMed
-
- US Renal Data System. USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2010.
-
- Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Hemmelgarn BR, Manns BJ, Lloyd A, et al. Relation between kidney function, proteinuria, and adverse outcomes. JAMA. 2010;303:423–439. - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108:2154–2169. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
