

Patients with heart failure in the "intermediate range" of peak oxygen uptake: additive value of heart rate recovery and the minute ventilation/carbon dioxide output slope in predicting mortality
- PMID: 22487616
- PMCID: PMC7240178
- DOI: 10.1097/HCR.0b013e31824f9ddf
Patients with heart failure in the "intermediate range" of peak oxygen uptake: additive value of heart rate recovery and the minute ventilation/carbon dioxide output slope in predicting mortality
Abstract
Purpose: While patients with heart failure who achieve a peak oxygen uptake (peak VO2) of 10 mL·kg(-1)·min(-1) or less are often considered for intensive surveillance or intervention, those achieving 14 mL·kg(-1)·min(-1) or more are generally considered to be at lower risk. Among patients in the "intermediate" range of 10.1 to 13.9 mL·kg(-1)·min(-1), optimally stratifying risk remains a challenge.
Methods: Patients with heart failure (N = 1167) referred for cardiopulmonary exercise testing were observed for 21 ± 13 months. Patients were classified into 3 groups of peak VO2 (≤10, 10.1-13.9, and ≥14 mL·kg(-1)·min(-1)). The ability of heart rate recovery at 1 minute (HRR1) and the minute ventilation/carbon dioxide output (VE/VCO2) slope to complement peak VO2 in predicting cardiovascular mortality were determined.
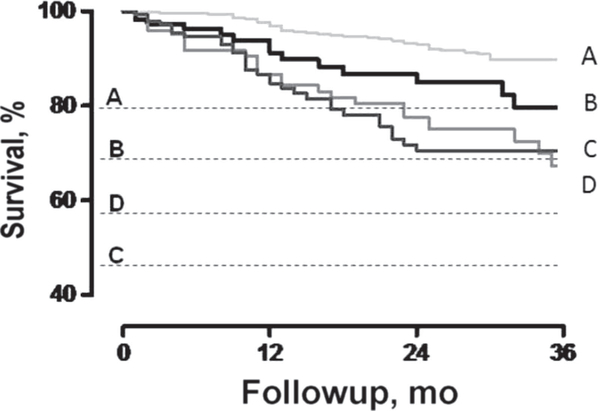
Results: Peak VO2, HRR1 (<16 beats per minute), and the VE/VCO2 slope (>34) were independent predictors of mortality (hazard ratio 1.6, 95% CI: 1.2-2.29, P = .006; hazard ratio 1.7, 95% CI: 1.1-2.5, P = .008; and hazard ratio 2.4, 95% CI: 1.6-3.4, P < .001, respectively). Compared with those achieving a peak VO2 ≥ 14 mL·kg(-1)·min(-1), patients within the intermediate range with either an abnormal VE/VCO2 slope or HRR1 had a nearly 2-fold higher risk of cardiac mortality. Those with both an abnormal HRR1 and VE/VCO2 slope had a higher mortality risk than those with a peak VO2 ≤ 10 mL·kg(-1)·min(-1). Survival was not different between those with a peak VO2 ≤ 10 mL·kg(-1)·min(-1) and those in the intermediate range with either an abnormal HRR1 or VE/VCO2 slope.
Conclusions: HRR1 and the VE/VCO2 slope effectively stratify patients with peak VO2 within the intermediate range into distinct groups at high and low risk.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guide-line update for the diagnosis and management of chronic heart failure in the adult: A report of the American College of Cardiology/American Heart Association in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation. Circulation. 2005;112:e154–e235. - PubMed
-
- Mehra MR, Kobashigawa J, Starling R, et al. Listing criteria for heart transplantation: International Society for Heart and Lung Transplantation guidelines for the care of cardiac transplant candidates—2006. J Heart Lung Transplant. 2006;25:1024–1042. - PubMed
-
- Mancini DM, Eisen H, Kussmaul W, et al. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation. 1991;83:778–786. - PubMed
-
- Myers J, Gullestad L, Vagelos R, et al. Cardiopulmonary exercise testing and prognosis in severe heart failure: 14 mL/kg/min revisited. Am Heart J. 2000;139:78–84. - PubMed
-
- Arena R, Myers J, Abella J, et al. Development of a ventilatory classification system in patients with heart failure. Circulation. 2007;115:2410–2417. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
