

Abnormal vital signs are strong predictors for intensive care unit admission and in-hospital mortality in adults triaged in the emergency department - a prospective cohort study
- PMID: 22490208
- PMCID: PMC3384463
- DOI: 10.1186/1757-7241-20-28
Abnormal vital signs are strong predictors for intensive care unit admission and in-hospital mortality in adults triaged in the emergency department - a prospective cohort study
Abstract
Background: Assessment and treatment of the acutely ill patient have improved by introducing systematic assessment and accelerated protocols for specific patient groups. Triage systems are widely used, but few studies have investigated the ability of the triage systems in predicting outcome in the unselected acute population. The aim of this study was to quantify the association between the main component of the Hillerød Acute Process Triage (HAPT) system and the outcome measures; Admission to Intensive Care Unit (ICU) and in-hospital mortality, and to identify the vital signs, scored and categorized at admission, that are most strongly associated with the outcome measures.
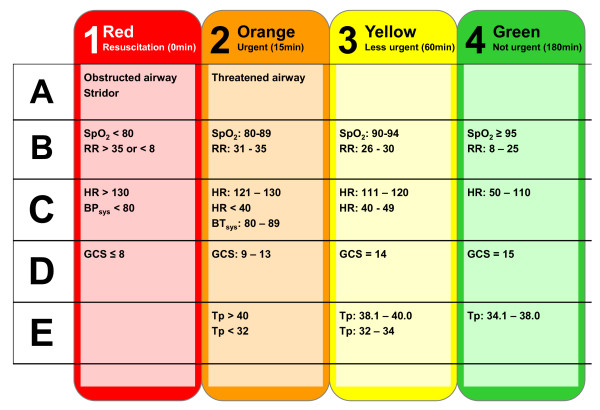
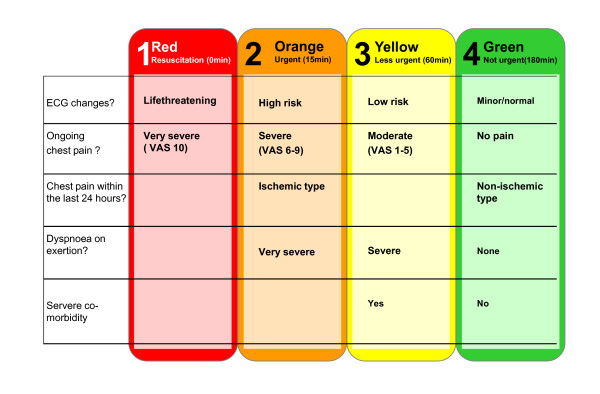
Methods: The HAPT system is a minor modification of the Swedish Adaptive Process Triage (ADAPT) and ranks patients into five level colour-coded triage categories. Each patient is assigned a triage category for the two main descriptors; vital signs, T(vitals), and presenting complaint, T(complaint). The more urgent of the two determines the final triage category, T(final). We retrieved 6279 unique adult patients admitted through the Emergency Department (ED) from the Acute Admission Database. We performed regression analysis to evaluate the association between the covariates and the outcome measures.
Results: The covariates, T(vitals), T(complaint) and T(final) were all significantly associated with ICU admission and in-hospital mortality, the odds increasing with the urgency of the triage category. The vital signs best predicting in-hospital mortality were saturation of peripheral oxygen (SpO(2)), respiratory rate (RR), systolic blood pressure (BP) and Glasgow Coma Score (GCS). Not only the type, but also the number of abnormal vital signs, were predictive for adverse outcome. The presenting complaints associated with the highest in-hospital mortality were 'dyspnoea' (11.5%) and 'altered level of consciousness' (10.6%). More than half of the patients had a T(complaint) more urgent than T(vitals), the opposite was true in just 6% of the patients.
Conclusion: The HAPT system is valid in terms of predicting in-hospital mortality and ICU admission in the adult acute population. Abnormal vital signs are strongly associated with adverse outcome, while including the presenting complaint in the triage model may result in over-triage.
Figures

References
-
- Eitel DR, Rudkin SE, Malvehy MA, Killeen JP, Pines JM. Improving service quality by understanding emergency department flow: a White Paper and position statement prepared for the American Academy of Emergency Medicine. J Emerg Med. 2010;38(1):70–79. doi: 10.1016/j.jemermed.2008.03.038. - DOI - PubMed
-
- Manchester Triage group. Emergency triage: Manchester Triage Group. London: BMJ Publishing Group, London, UK; 1997.
-
- Beveridge R, Clarke B, Janes N. Canadian emergency department triage and acuity scale; implementation guidelines. Can J Emerg Med. 1999;1:2–28.
-
- Lethvall S. ADAPT - Adaptiv Processtraige/VITALHISTORIER. Version 1.1.2008. Giltiga 080424-090531 (Sweden)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
