

Oral nystatin prophylaxis in surgical/trauma ICU patients: a randomised clinical trial
- PMID: 22490643
- PMCID: PMC3681386
- DOI: 10.1186/cc11300
Oral nystatin prophylaxis in surgical/trauma ICU patients: a randomised clinical trial
Abstract
Introduction: Candida prophylaxis in ICU is still a matter of debate. Oral chemoprophylaxis has been advocated to reduce the incidence of Candida colonisation and infection.
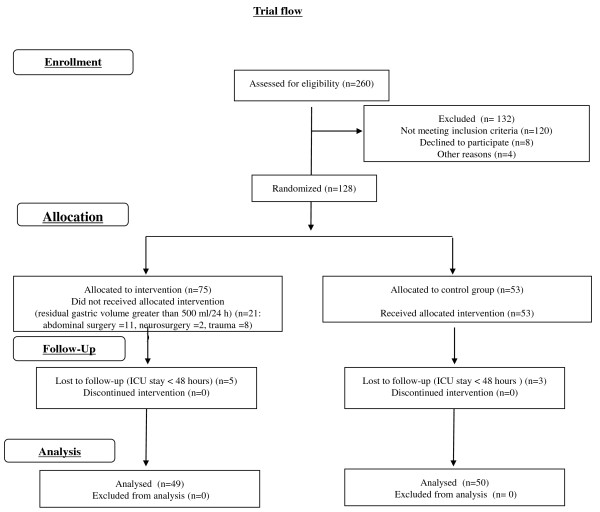
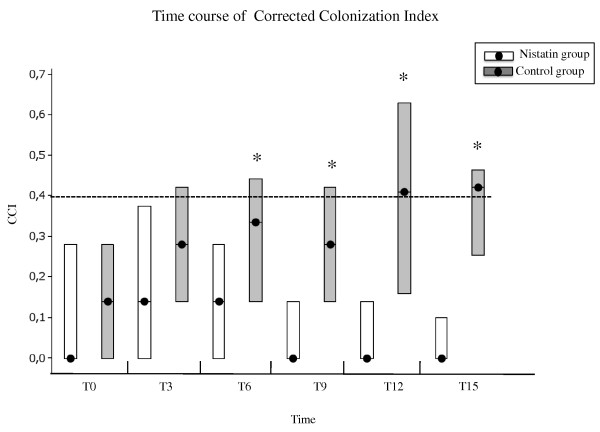
Methods: We performed a randomised trial studying a single drug (nystatin) versus control in surgical/trauma ICU patients. Multiple-site testing for fungi was performed in each patient on ICU admission (T0) and subsequently every 3 days (T3, T6, T9, and so forth). The primary evaluation criterion was the time course of the corrected colonisation index.
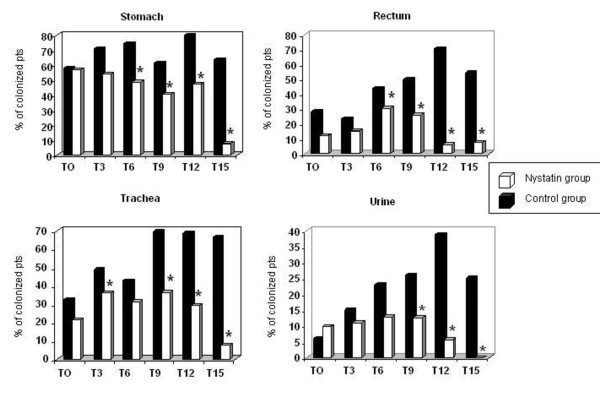
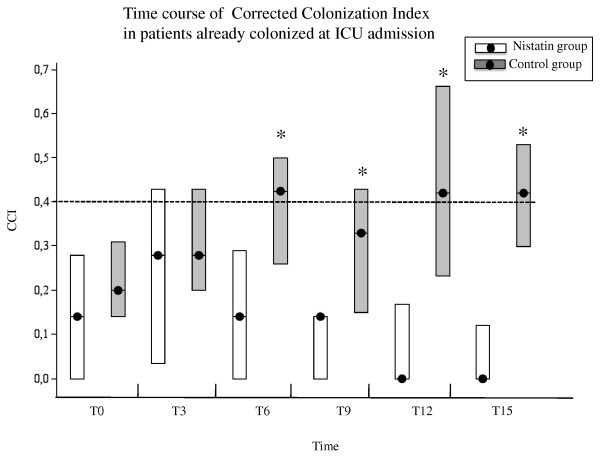
Results: Ninety-nine patients were enrolled. At admission, 69 patients exhibited Candida colonisation: the most frequently colonised body sites were the stomach and the pharynx. The most frequent isolated species was Candida albicans. The corrected colonisation index was similar in the two groups at T0 (P = 0.36), while a significant statistical difference was observed between the treatment and control groups at T6 (median 0.14 and 0.33, respectively; P = 0.0016), at T9 (median 0.00 and 0.28, respectively; P = 0.0001), at T12 (median 0.00 and 0.41, respectively; P = 0.0008), and at T15 (median 0.00 and 0.42, respectively; P < 0.0003). The same results were obtained in the subgroup of patients already colonised at ICU admission.
Conclusion: This trial shows that nystatin prophylaxis significantly reduces fungal colonisation in surgical/trauma ICU patients, even if already colonised.
Trial registration: ClinicalTrials.gov: NCT01495039.
Figures
Comment in
-
Impact of nystatin on Candida and the oral microbiome.Crit Care. 2012 Jul 23;16(4):440; author reply 440. doi: 10.1186/cc11360. Crit Care. 2012. PMID: 22827886 Free PMC article. No abstract available.
-
Topical nystatin prophylaxis: a likely viable measure for reducing impact of candidemia in neurosurgical patients with early tracheostomy intubation.Crit Care. 2013 Feb 18;17(1):414. doi: 10.1186/cc11921. Crit Care. 2013. PMID: 23414732 Free PMC article. No abstract available.
-
Topical nystatin prophylaxis: a likely viable measure for reducing impact of candidemia in neurosurgical patients with early tracheostomy intubation. Author's response.Crit Care. 2013;17(1):414. Crit Care. 2013. PMID: 25237682 No abstract available.
References
-
- Olaechea PM, Palomar M, León-Gil C, Alvarez-Lerma F, Jordá R, Nolla-Salas J, León-Regidor MA. EPCAN Study Group. Economic impact of Candida colonization and Candida infection in the critically ill patient. Eur J Clin Microbiol Infect Dis. 2004;16:323–330. doi: 10.1007/s10096-004-1104-x. - DOI - PubMed
-
- Tortorano AM, Peman J, Bernhardt H, Klingspor L, Kibbler CC, Faure O, Biraghi E, Canton E, Zimmermann K, Seaton S, Grillot R. ECMM Working Group on Candidaemia. Epidemiology of candidaemia in Europe: results of 28-month European Confederation of Medical Mycology (ECMM) hospital-based surveillance study. Eur J Clin Microbiol Infect Dis. 2004;16:317–322. doi: 10.1007/s10096-004-1103-y. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
